
Scan Less, Think More: Canadian Rules for Head and C-Spine Trauma
Hello All,
Quick notes from last night.
CT Head Imaging
"Head trauma without brain injury" and mild/minor traumatic brain injury are clinical diagnoses.
Caution is advised to avoid overuse of CT imaging, especially in young patients who are not on anticoagulation.
Remember, CT imaging is not benign. It is associated with radiation and increased cancer risk, cost to the patient, and hospital resource utilization (CT table, radiology reading, tech availability etc.)
A validated decision aid or guideline can be used in the appropriate population to determine necessity to avoid unnecessary imaging.
High sensitivity (95%-100%) and specificity (35%-65%).
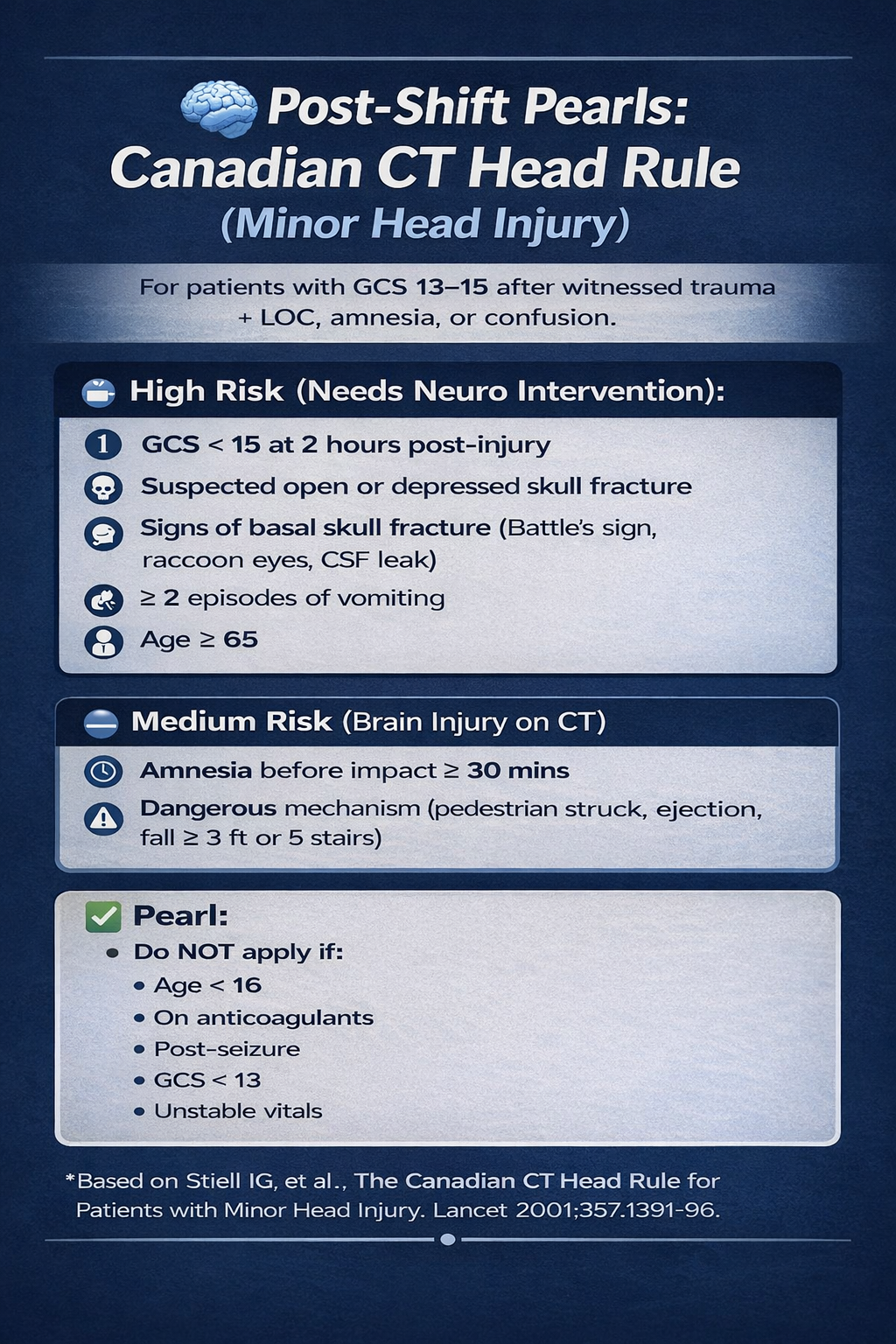
INCLUSION CRITERIA: Patients with GCS scores of 13-15 AND at least one of the following: LOC, amnesia to the head injury event, or witnessed disorientation.
This is important. "I hit my head" does not equal "CT Scan"
Just because the patient bumps their head does not mean they enter this pathway. If the patient did not lose consciousness, remembers everything, and is GCS15...don't pass go. Don't scan them. They are going to be okay.
Inappropriate application of this tool decreases its specificity.
Exclusion criteria: individuals <16 years old, patients on blood thinners, and those who had a seizure after injury.
2. C-Spine Imaging
Will reiterate the above. Caution is advised to avoid overuse of CT imaging, especially in young patients. Remember, CT imaging is not benign.
Maintains high sensitivity but increases specificity when compared to NEXUS decision rule.
Canadian C-Spine: Sensitivity 99.4% (95% CI, 96%-100%), Specificity 45.1% (95% CI, 44%-46%)
NEXUS: Sensitivity 99.6% (95% CI, 98.6%-100%), Specificity 12.9 % (95% CI, 12.8%-13.0%)
If a patient has any high-risk factors (age ≥65, a defined dangerous mechanism or paresthesias in the arms or legs) then they require c-spine imaging.
If a patient has no high-risk factors but meets none of the defined low risk criteria (see list), they require c-spine imaging.
If a patient has no high risk factors, has neck pain, but meets even one low risk factor, then it is safe to assess whether the patient is able to rotate their neck 45 degrees to the left and right.
If they can do this (even with some pain or discomfort), then they do not require further imaging. If they cannot rotate their neck 45 degrees in both directions then c-spine images are indicated.
Note that this rule allows you to avoid C-spine imaging even if the patient is "tender" in their midline if they have another low risk factor present. It allows you to also to avoid the subject nature of intoxication and distracting injury of NEXUS.
My own (evidence-based) C-spine clearance strategy. Remember, you only need ONE low-risk factor to move on to neck rotation assessment.
Listen to this cool FOAMCAST episode that discusses C-spine imaging decision tools and cervical spine clearance.
It reviews the updated guidance and evidence from specialty organizations (Trauma EAST, ACR)
Evidence suggests that we can clear the C-collar of intoxicated or obtunded patients due to the very low risk of missed, clinically significant C-spine injury.
Evidence also suggests that patients with "midline tenderness" and a negative CT can also be cleared due to the very low risk of missed, clinically significant C-spine injury.
Neurologic deficits are what matter!
Cheers,
Dillon