
Welcome to The Pearl Log — where post-shift wisdom surfaces, one shiny clinical take at a time. Some pearls are fresh, some are rough, all are found under pressure.
Find a Pearl

Deep Dive: ED Hip Fracture Management
A practical review of ED management of hip fractures, including high-yield bedside pearls, occult fractures, peripheral nerve blocks, and communicating with orthopedics. It also takes a closer look at the evidence behind preoperative Buck's traction and what current guidelines recommend.

Tizanidine Overdose and Hyperemesis Gravidarum
A brief discussion on tizanidine overdose management and hyperemesis gravidarum.
Quick Hits: Airway update, headache guidelines, status epilepticus, nailbed repair, and shellfish allergies.
Several topics we discussed on shift, including evidence-based airway management, rapid treatment of status epilepticus, nail bed injury management after the NINJA trial, contemporary migraine therapy, and the persistent myth surrounding shellfish allergy and iodinated contrast. As always, these are meant to be quick introductions to practice-changing literature and resources that are worth a closer look.
Chest Pain, Anticoagulated Falls, and Bug Bites
Explore how prevalence shapes chest pain risk, why CT decisions in anticoagulated falls remain an evidence gap, and how large local allergic reactions can convincingly masquerade as cellulitis.

Enough is Enough. Routine Coags in the ED.
Routine coags in low-risk ED patients rarely change management and often create downstream problems instead.

Aortas, Rectums, and BPPV
A little bit on suprasternal notch view for aortic dissection, the importance of the digital rectal exam for perirectal abscess diagnosis, and a referral to a new BPPV review article.

Leg Pain Pontification
Osteoarthritis is a clinical diagnosis driven by multifactorial structural and central pain mechanisms, where symptom severity often poorly correlates with imaging, and management remains stepwise with a focus on nonpharmacologic therapy and, if needed, topical NSAIDs. For suspected DVT, a structured approach using Wells criteria and age-adjusted D-dimer safely reduces unnecessary imaging, with recent prospective data supporting its reliability in low- to moderate-risk patients.

Knee Pain and Monkeypox
Throw out those knee immobilizers for traumatic knee pain.
Don’t miss monkeypox when it walks into your ER!
Quickhits: Whole Blood In Trauma, Triple Negative Breast Cancer, and the Linear Probe for IUP
Whole blood for trauma, triple negative breast cancer, and ultrasound for IUP identification.

Early Pregnancy Loss in the Emergency Department
Early pregnancy loss is common and requires careful diagnosis using strict ultrasound criteria before confirming nonviability. Stable patients should be offered all three management options—expectant, medical, and procedural—with medical therapy using mifepristone and misoprostol as an effective, evidence-based approach. Most cases can be managed with clinical follow-up rather than routine imaging, with clear return precautions and patient-centered counseling guiding safe disposition.

2026 AHA Guideline on Acute Pulmonary Embolism
The 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for Evaluation and Management of Acute Pulmonary Embolism. A brief ED focused summary.


Post Cardiac Arrest Management
The AHA has put out a bunch of recent statements and guidelines regarding post cardiac arrest care. Take a look at these to up your game!

Migraine Headache Pathophys + Diagnosis
Migraine is a primary disorder of neuronal dysfunction, driven by abnormal brain excitability and dysregulated pain modulation. Cortical spreading depression and trigeminovascular activation lead to CGRP-mediated neurogenic inflammation and progressive sensitization, leading to aura, headache pain, and associated symptoms. This modern framework clarifies why migraine presents in predictable phases and why early, mechanism-targeted treatment in the ED matters.
Atrial Fibrillation Guideline Check-In
Despite differences across AF guidelines, ED management converges on three principles: initiate DOACs when stroke risk warrants, cardiovert fewer patients but with more attention to duration and risk, and ensure early referral for rhythm-control discussion in newly diagnosed AF. The ED role is less about choosing the “right” guideline and more about safe initiation, thoughtful restraint, and reliable follow-up.

Subclavian CVCs
Subclavian access offers durability and lower infection risk but demands respect for nearby pleura and artery. Ultrasound guidance reduces complications, with infraclavicular and supraclavicular approaches offering different ergonomic and anatomic advantages. Landmark technique remains a valid option when speed, experience, or resource constraints matter.
Out of Breath? Inpatient-Bound CAP Treatment
Inpatient CAP management hinges on severity. Use validated IDSA/ATS criteria to guide ICU vs ward disposition, but most severe and non-severe cases get similar empiric antibiotics like a beta-lactam plus macrolide or a fluoroquinolone. Reserve MRSA or Pseudomonas coverage for true risk factors, skip routine anaerobic coverage for aspiration unless abscess or empyema is suspected, and remember newer data support steroids and HFNC in severe hypoxic CAP.

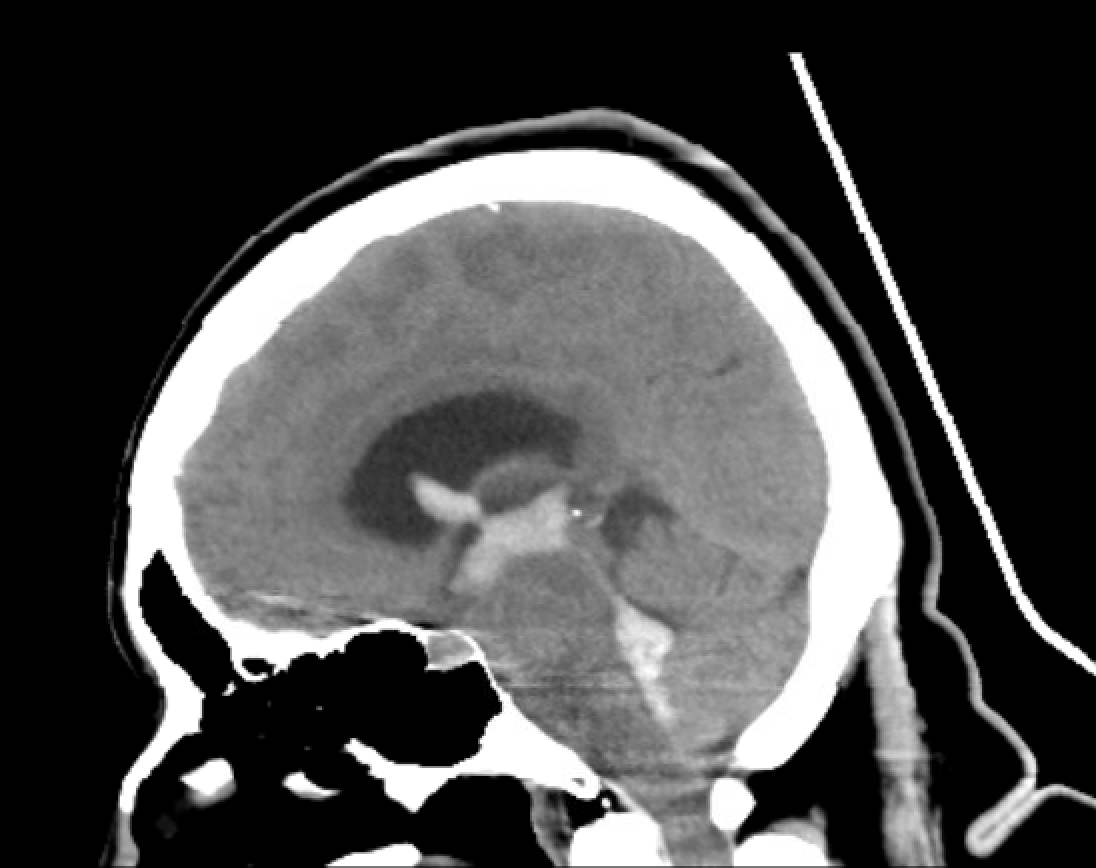
a BIG Deal.
The Brain Injury Guidelines provide an evidence-based framework to safely risk stratify patients with blunt traumatic brain injury and intracranial hemorrhage. By incorporating clinical context alongside imaging findings, mBIG helps reduce unnecessary neurosurgical consultations, repeat CT scans, and admissions. Implementation should remain institution-specific and grounded in clinical judgment and system capabilities.

Scan Less, Think More: Canadian Rules for Head and C-Spine Trauma
A quick review and commentary on the Canadian CT head and CT C-Spine clinical decision rules.