
a BIG Deal.
Hi everyone,
Today is all about a high-level review of the Brain Injury Guidelines (BIG)/Modified BIG (mBIG). These guidelines are designed to help us manage blunt traumatic brain injury more thoughtfully, with an emphasis on safety, efficiency, and avoiding unnecessary resource use. The term has been thrown around much more frequently in recent months, so it's worth a dedicated review.
The Big Picture
The Brain Injury Guidelines (BIG) were developed to guide more effective resource utilization in patients with blunt traumatic brain injury
The goal was to reduce:
Unnecessary transfers
Routine neurosurgical consultation
Repeat CT imaging in patients unlikely to require intervention
Originally published in 2014, with several external validations, including a large multi-institutional prospective validation published in 2022
Modified BIG (mBIG) was subsequently developed to refine the original framework to improve:
Reproducibility
Patient safety
Consistency in real-world application
How mBIG Works
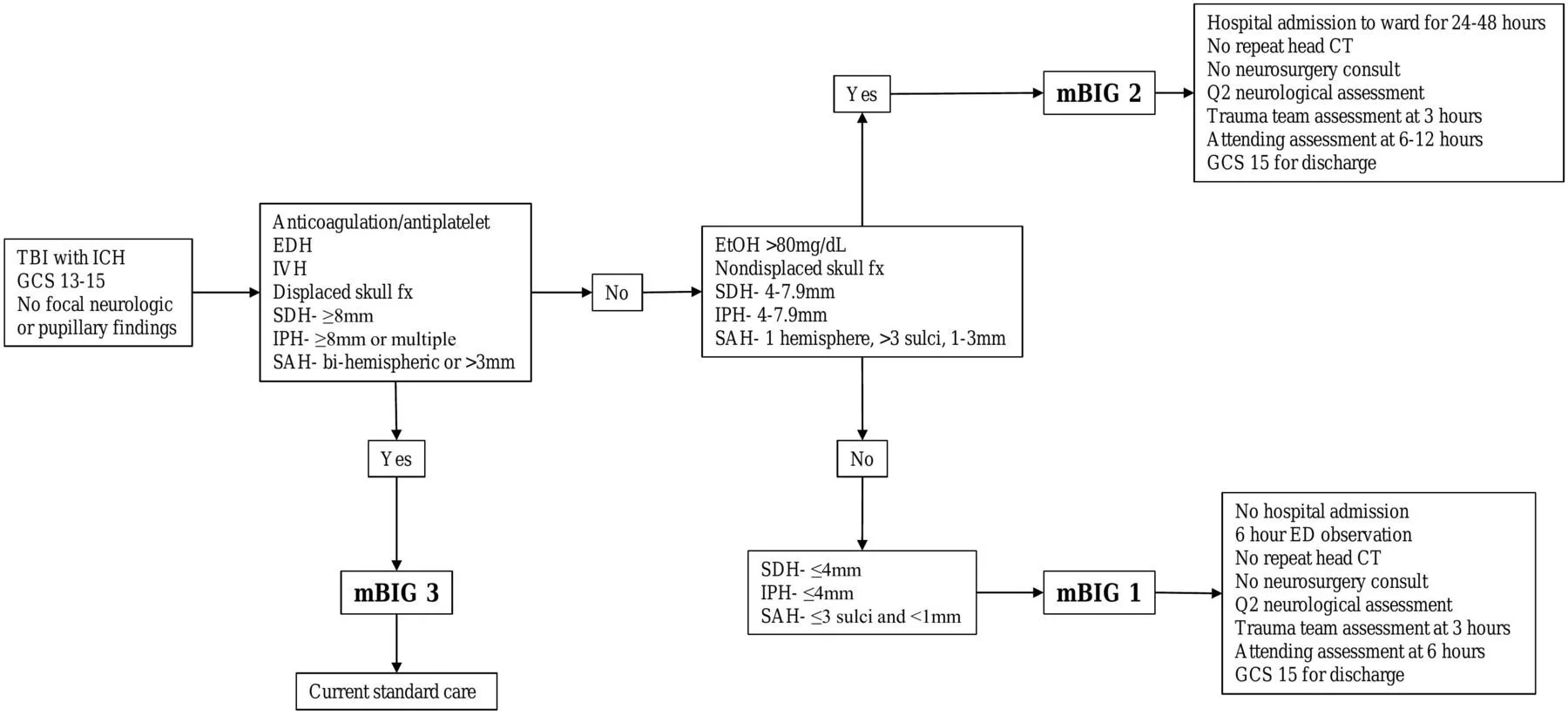
Under mBIG, patients with TBI and intracranial hemorrhage are stratified into three categories: mBIG 1, mBIG 2, mBIG 3.
Classification is based on:
Clinical presentation and neurologic exam
Radiographic characteristics of the intracranial hemorrhage
Additional patient factors that affect risk and safety
mBIG emphasizes clinical context plus imaging to guide disposition and management.
Practical ED Management Framework
mBIG 1
Short ED observation for 6 hours with q2hr neurologic assessments
No routine repeat head CT
No required neurosurgical consultation
Discharge if neurologically stable at 6 hours
mBIG 2
Hospital admission for observation
No routine repeat head CT
Neurosurgical consultation not routinely required
mBIG 3
"The Standard of Care", including hospital admission, neurosurgical consultation, and likely repeat imaging often appropriate
Don't worry, MDCALC has your back on this. But it's important to understand this, not just plug and chug.
The key idea is that not all intracranial hemorrhages need the same intensity of care.
Important Limitations
mBIG is a head injury guideline, not a global disposition rule
Patients with significant medical comorbidities may still require admission
Always zoom out and ask:
Why did this patient fall?
Was the injury a consequence of another acute illness?
A patient can meet mBIG 1 or 2 criteria and still need admission for medical reasons unrelated to the head injury itself.
Evidence and External Validity
Multiple validation studies have shown reassuring safety outcomes
A common criticism is that much of the data comes from Level 1 trauma centers
Applicability may be more limited in:
Rural settings
Resource-limited hospitals
Environments where return to care after deterioration is difficult
Local context matters when applying these guidelines.
Neurosurgery Involvement: Real-World Considerations
In some institutions, it may be unrealistic to avoid neurosurgical consultation entirely
Even with neurosurgery-driven mBIG pathways, studies show:
Improved discharge rates
Fewer repeat neuroimaging studies
Better standardization of care
Early neurosurgical involvement may also:
Facilitate outpatient follow-up
Reduce delays if deterioration occurs
The biggest gains may come from shared expectations and agreed-upon pathways, not from excluding consultants altogether.
Bottom Line
mBIG provides a structured, evidence-based approach to managing blunt TBI
It can safely reduce unnecessary imaging, consultations, and admissions
Implementation should be institution-specific, accounting for:
Available resources
Transport considerations
Local practice culture
The most effective approach is coordinated planning between the ED, trauma team, and neurosurgery.
Key Takeaways
Not all intracranial hemorrhages need repeat CTs or neurosurgical consults
Clinical stability matters as much as CT findings
mBIG guides disposition related to head injury management, but may not be the final word.
Local context and systems of care should drive how these guidelines are applied
Further Reading & Resources
Cheers,
Dillon