
Out of Breath? Inpatient-Bound CAP Treatment
Hey Team,
Today, let’s chat briefly about inpatient treatment of community-acquired pneumonia. I would recommend a review of the 2019 IDSA/ATS guidelines. Reviewing consensus guidelines can be helpful, and definitely reminded me of a few key components of inpatient therapy. Additional information can be found on EMCRIT, particularly on the discussion of steroid use in CAP.
Source: Metlay, J. P., et al. (2019). Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. American journal of respiratory and critical care medicine, 200(7), e45–e67. [PubMed]
Several Key Points:
Severity of pneumonia dictates disposition. Severe pneumonia should generally go to the ICU. Although they have been in use since 2007, these IDSA/ATS criteria have been repeatedly validated for use in triage to the ICU vs ward.
Specifically, they recommend:
Direct admission to an ICU for patients with hypotension requiring vasopressors or respiratory failure requiring mechanical ventilation (strong recommendation, low quality of evidence).
Using the IDSA/ATS 2007 minor severity criteria together with clinical judgment to guide the need for higher levels of treatment intensity (conditional recommendation, low quality of evidence).

Metlay et al. 2019
2. Severe and Non-Severe PNA can be treated with similar antibiotic regimens in most situations.
Beta-Lactam + Macrolide or a Fluoroquinolone
ie: CTX + Azithromycin
3. Expanded coverage for MRSA (Vancomycin) or Pseudomonas (Cefepime, Pip-Tazo) is based on predefined risk factors for MRSA/Pseudomonas.
Debate on whether ICU admission itself is a risk factor that warrants vancomycin coverage until MRSA screening results return.
The most consistently strong individual risk factors for respiratory infection with MRSA or P. aeruginosa are prior isolation of these organisms, especially from the respiratory tract, and/or recent hospitalization and exposure to parenteral antibiotics. Other risk factors are less strongly associated with these infections.
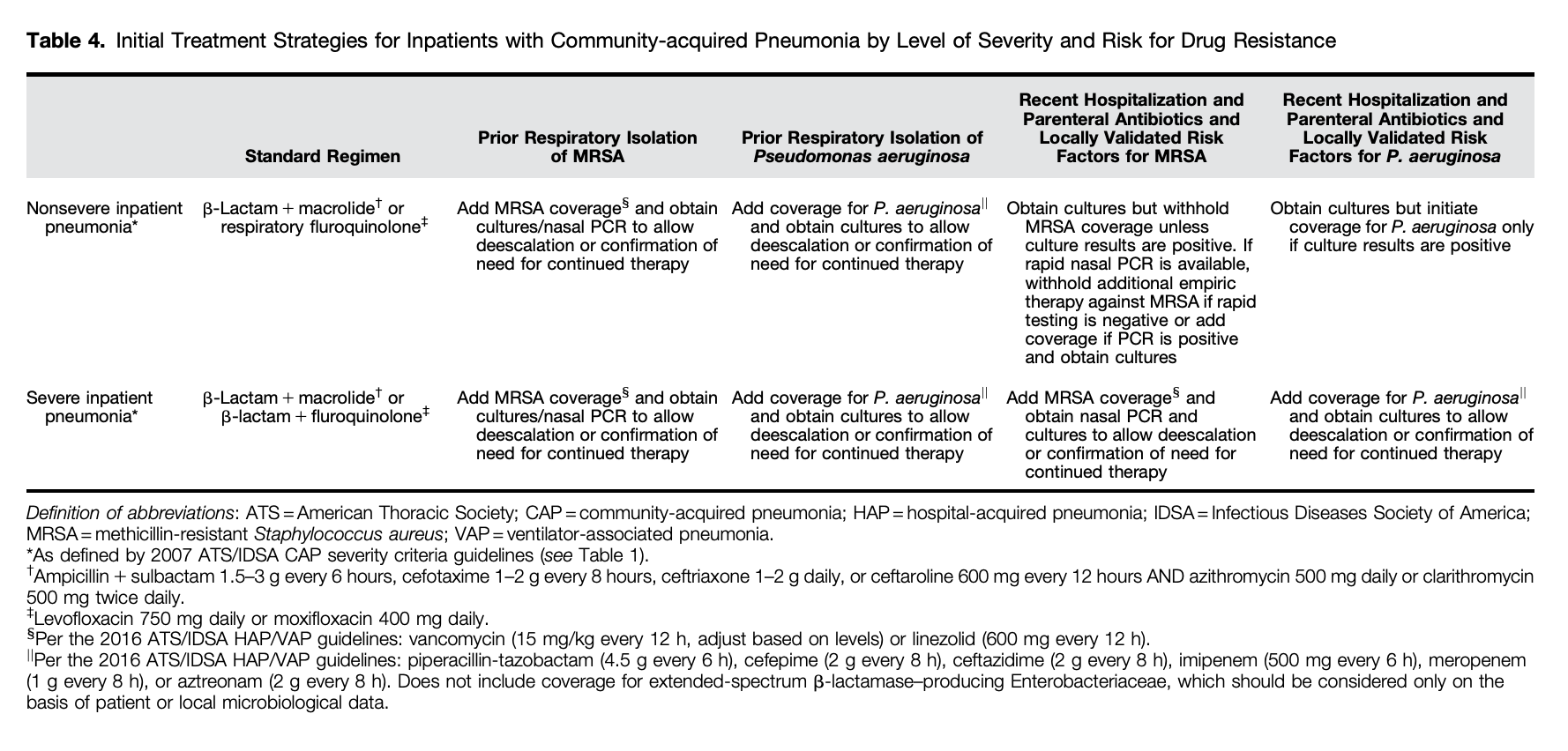
Metlay et al, 2019.
4. Anaerobic coverage is not recommended for “aspiration” pneumonia.
They suggest routinely NOT adding anaerobic coverage for suspected aspiration pneumonia unless lung abscess or empyema is suspected (conditional recommendation, very low quality of evidence).
This also means that if pneumonia is your most likely diagnosis, it is likely better to use Cefepime over Pip-Tazo for pseudomonal coverage in the critically ill.
Caution: If you are treating a critically ill patient (hypotensive, shocky, intubated, etc) and the diagnosis is uncertain, as the ED doc…don’t get “too fancy”, and go broad while the work-up is ongoing.
5. NEW SINCE 2019 IDSA/AST GUIDELINES: STEROIDS IN SEVERE CAP
Since these guidelines were published, more data have been published supporting the use of corticosteroids in severe CAP.
The CAPECOD Trial published in NEJM in 2023 found that among patients with severe community-acquired pneumonia being treated in the ICU, those who received hydrocortisone had a lower risk of death by day 28 than those who received placebo.
You will see they used 200 mg hydrocortisone daily by continuous IV infusion as their intervention.
A pragmatic, accepted alternative is 50 mg hydrocortisone q6h.
6. High Flow Nasal Cannula
The FLORALI Trial published in the NEJM of medicine in 2015, in patients with nonhypercapnic acute hypoxemic respiratory failure (majority Pneumonia), treatment with high-flow oxygen, standard oxygen, or noninvasive ventilation did not result in significantly different intubation rates. There was a significant difference in favor of high-flow oxygen in 90-day mortality.
EMCRIT talks about this further and recommends HFNC as first line for acute hypoxic (but not hypercapneic) respiratory failure.
Other things I’m listening to:
Cheers,
Dillon