
Intraventricular Hemorrhage
Hello Team,
Let's chat about a topic from last shift.
Primary Intraventricular Hemorrhage (pIVH)
Primary intraventricular hemorrhage is uncommon, easy to miss, and dangerous mostly because it can cause rapid obstructive hydrocephalus and increased intracranial pressure (ICP). The “stroke-like deficit” picture is often not the main feature. Think pressure physiology.
Definition
Primary intraventricular hemorrhage (pIVH) is isolated bleeding into the ventricular system that arises from a structure within or adjacent to the ventricles, without a primary intraparenchymal hemorrhage that secondarily extends into the ventricles.
Epidemiology and Etiology
Rare: about 3% of non-traumatic intracranial hemorrhage
A meaningful portion is cryptogenic (no identifiable cause despite workup)
Reported contributors and associated etiologies include:
Hypertension (likely a leading hypothesis in many cryptogenic cases)
AVM
Moyamoya
Coagulopathy / anticoagulation
Choroid plexus tumor or other intraventricular lesions (less common)
Pathophysiology
Blood within the ventricular system can impair CSF flow and absorption, causing:
Obstructive hydrocephalus
Acute rise in ICP
Secondary neurologic injury from hypoxemia, hypo-/hyper-tension, dyscarbia, hyperthermia, and sympathetic surges (especially around intubation)
Clinical Presentation
Most presentations reflect sudden increased ICP:
Abrupt headache
Nausea, vomiting
Confusion, disorientation
Decreased level of consciousness
Pearl: Up to ~25% may have progressive or fluctuating onset rather than purely thunderclap.
Neuro exam pattern:
Focal deficits are relatively uncommon in pIVH.
If present, can reflect ICP effects (for example, cranial nerve palsies, especially 6th nerve).
Diagnosis and Initial Imaging
Non-contrast head CT is the first test
Shows hyperdensity within ventricles consistent with acute blood
Evaluates for:
Hydrocephalus
Associated parenchymal hemorrhage (helps distinguish primary vs secondary IVH)
Subarachnoid hemorrhage

Noncontrast CTH, Axial View. See hyperdensity in the lateral ventricles. Note the absence of intraparenchymal hemorrhage.
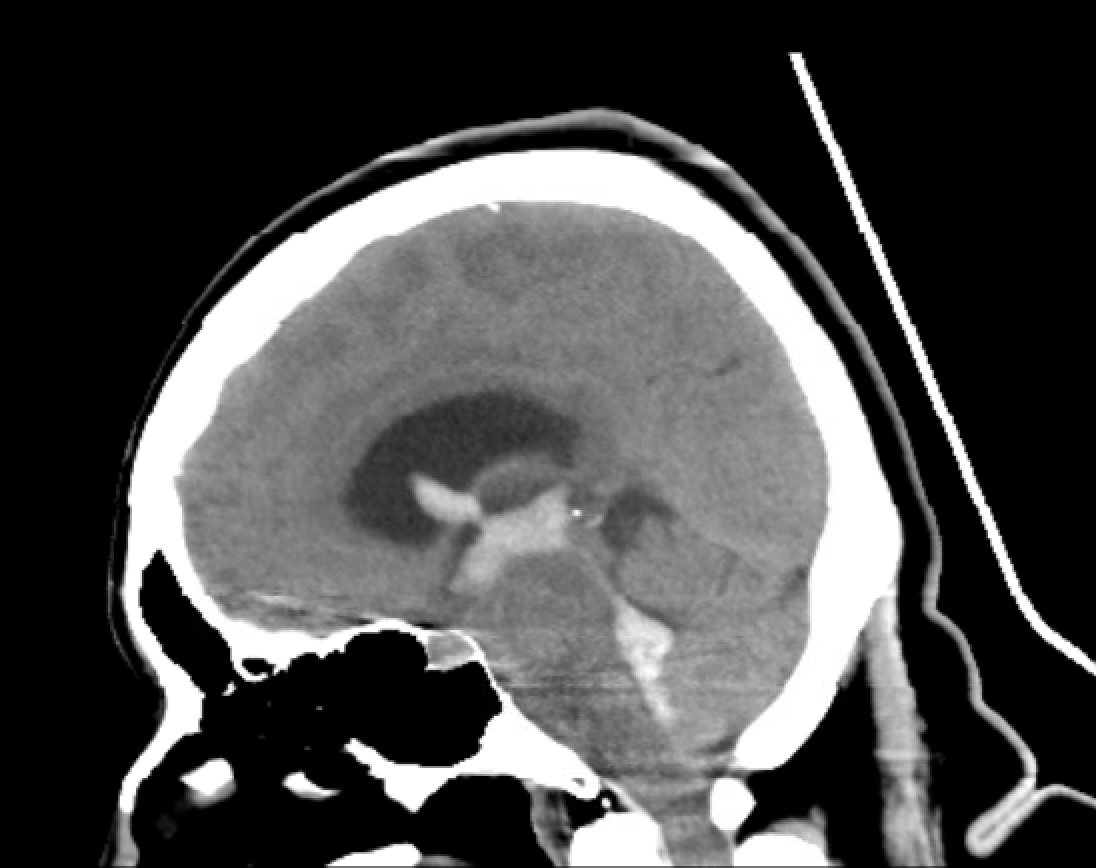
Noncontrast CT Head, Sagittal View: See extensive hyperdensities that extend from the 4th ventricle, through the 3rd ventricle, to the lateral ventricles.
Core ED Management Priorities
Stop or limit ongoing bleeding
Monitor for hydrocephalus and neurologic deterioration
Treat underlying cause when present
Prevent secondary brain injury
Anticoagulation reversal: If anticoagulated: reverse. This is a bleed where reversal is strongly indicated.
Blood pressure management is a balancing act:
Lower BP may reduce risk of expansion
But excessive lowering can reduce cerebral perfusion pressure, especially if ICP is elevated
Practical approach (consistent with ICH management principles, though data for pIVH is limited):
Target systolic BP roughly 130–150 (AHA/ASA recommendations)
Common IV options:
Clevidipine (very titratable, short half-life)
Nicardipine (widely available, effective, watch overshoot)
Labetalol (bolus option)
Others depending on local practice
Hydrocephalus Watch
High-risk ventricles: Blood in the 3rd or 4th ventricle increases risk of obstructive hydrocephalus.
Obstructive hydrocephalus can be rapidly fatal via herniation physiology.
Actions:
ICU-level monitoring
Repeat imaging if neuro status worsens
If obstructive hydrocephalus develops: external ventricular drain (EVD) by neurosurgery is definitive temporizing therapy.
Prognosis and Complications
Prognosis varies with severity, bleed burden, complications, and baseline function.
Reported in-hospital mortality: ~20–50%
Long-term complications can include:
Neurocognitive sequelae
Non-communicating hydrocephalus
Late recurrence of bleeding
Airway and Intubation in Acute Brain Injury
Goal: avoid secondary brain injury during airway management.
Before intubation
Do as complete a neuro exam as possible: GCS, Pupils and reactivity, Motor exam, posturing, localization, midline crossing if applicable
Preoxygenate aggressively
Set up apneic oxygenation
During intubation
Core goals:
Maximize first-pass success
Avoid hypoxemia and hypercapnia
Target eucapnia even during BVM
Technique:
RSI with video laryngoscopy is best approach due to evidence for 1st pass success
Pretreatment option:
Fentanyl 2–3 mcg/kg can blunt sympathetic response to laryngoscopy in select stable patients, but requires time (a few minutes) and readiness for possible apnea.
Induction agent:
Prefer hemodynamically neutral agents like etomidate or ketamine
Ketamine is acceptable and does not meaningfully increase ICP
Paralytic:
Succinylcholine is attractive due to rapid on/off for serial neuro exams
Theoretical transient ICP increase due to fasciculation is debated and data quality is limited. Weigh this against the real benefit of short duration.
After intubation
Target homeostasis (normoxia, eucapnia, normotension)
Hyperventilation is a rescue maneuver, not routine
Analgesia first-line: short-acting opioids (fentanyl)
Sedation: propofol for titratability and short half-life, but watch hypotension
Common pitfall:
Starting sedation/analgesia and an antihypertensive drip simultaneously. Treat pain/anxiety first, reassess BP, then titrate antihypertensive.
In a similar vein, don’t reflex-start an antihypertensive drip before treating pain/anxiety and before induction if you can avoid it. Peri-intubation hypotension is real.
Managing Increased ICP
First-line: positioning and ensuring venous drainage
Head of bed 30 degrees
Neck midline
Remove avoidable neck obstruction (for trauma, clear collar when appropriate based on imaging and institutional practice)
Physiologic targets
Normoxia
Eucapnia
Normothermia
Hemodynamic stability (avoid hypotension; avoid extreme hypertension)
Hyperosmolar therapy
If ongoing signs of elevated ICP despite basics:
3% hypertonic saline (e.g. 250 mL over 10–15 min)
If 3% not immediately available:
Consider sodium bicarbonate pushes as a practical alternative in a pinch (1–2 amps over ~10 minutes as a rough substitute)
Mannitol not as favorable due to risk of hypotension (especially in trauma)
References
1) Hoyne J, Edlow J. Here’s My Take: Airway Management in Patients With Acute Brain Injury or Ischemia
The Journal of Emergency Medicine. 2025;74:125-133.
https://doi.org/10.1016/j.jemermed.2024.12.015
ScienceDirect Link
2) UpToDate. Intraventricular hemorrhage (clinical topic review)
UpToDate. (Accessed 2026).
UpToDate Intraventricular hemorrhage — clinical review
3) EMCrit IBCC: Intracerebral Hemorrhage (ICH/IVH Section)
EMCrit Intelligent Board-Certified Critical Care.
EMCrit ICH/IVH page
What I'm reading/listening:
Cheers,
Dillon