
A Scary EKG
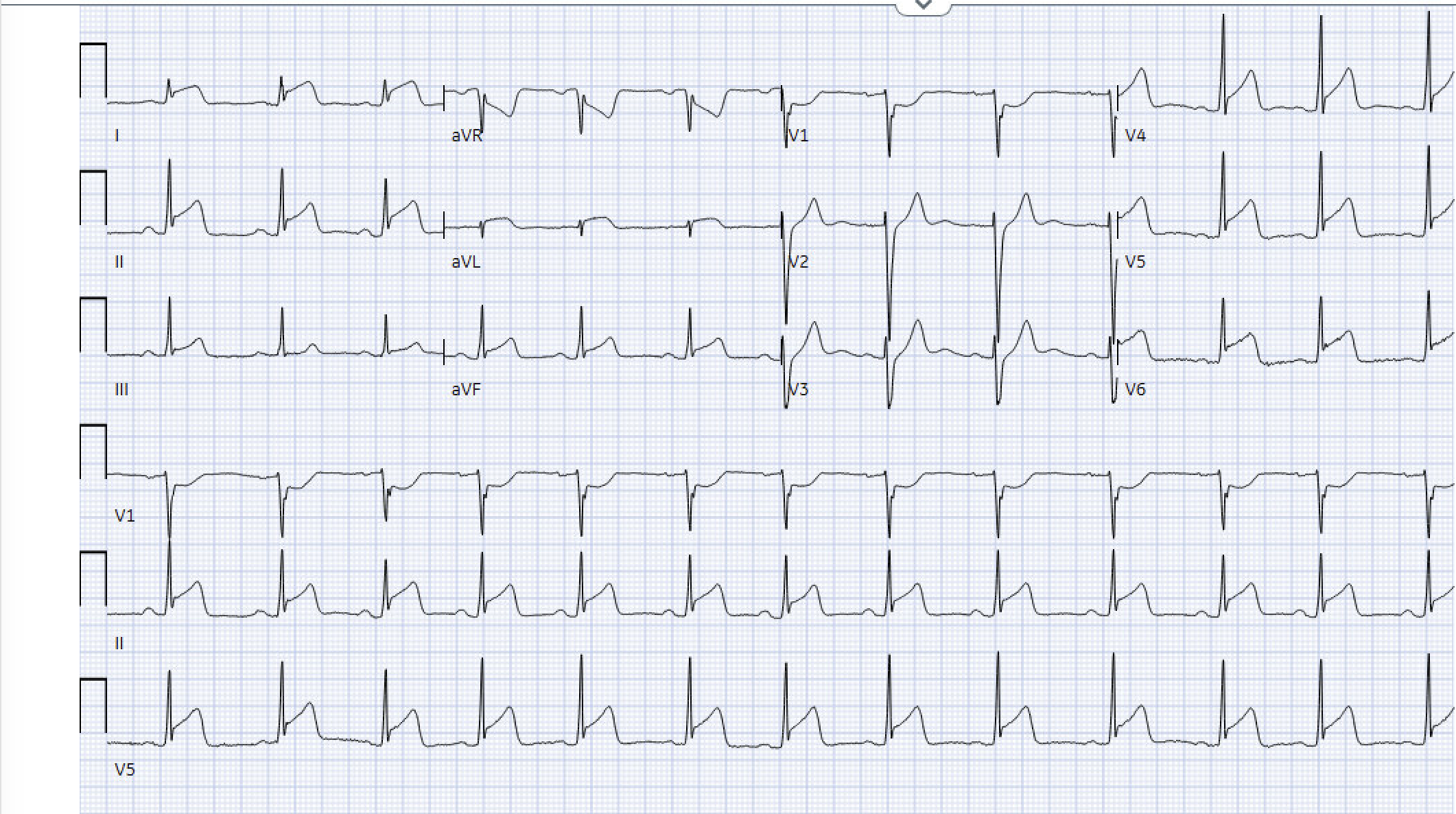
You are handed a triage EKG on a 26-year-old man who just re-registered for chest pain.
- STOP -
What would you do with this EKG? Would you activate the cath lab? Would you room the patient emergently? What other information would you want to know? Why did you make this decision?
~Clinical Reasoning Time~
Let’s chat about the rest of his ED course:
This was a 26-year-old man with no medical history who returned to the ED with persistent chest pain after discharge the prior day following a negative CTA aorta and normal troponin. He described a diffuse, burning chest pain that was possibly worse when supine and improved when upright, but not a slam dunk. He denied fever, recent URI symptoms, palpitations, exertional pain, substance use, or family history of early CAD or thromboembolic disease.
A triage EKG prompted immediate rooming. He was hemodynamically stable with normal vital signs. Exam was notable for discomfort but no friction rub, normal breath sounds, and was otherwise unremarkable.
The EKG pattern raised concern for myopericarditis, but the diagnosis felt hesitant rather than settled given how dramatic the tracing was. Bedside ultrasound showed no pericardial effusion and reassuringly no obvious regional wall motion abnormality. At that point, all we had was chest pain and the EKG.
Inflammatory markers returned elevated with a CRP of 61.2, followed by a critically elevated troponin of 17.7, which escalated concern despite the overall presentation. While myocarditis can cause significant troponin elevation, so can ACS. Cardiology was consulted immediately. Although the ECG pattern and clinical context favored myopericarditis, cardiology elected to activate the cath lab given the degree of troponin elevation and evolving ECG changes. The patient was started on heparin and taken emergently for coronary angiography.
Cardiac catheterization revealed clean coronaries. Formal echocardiography revealed normal ventricular function and no pericardial effusion. Cardiac MRI remains pending.
Differentiating STEMI from Acute Pericarditis on the EKG
* Quick Reminder: EKG changes imply epicardial inflammation since the parietal pericardium itself is electrically inert. These EKG changes are attributed to repolarization abnormalities of the atrial and ventricular myocardium in response to epicardial inflammation.
Stepwise approach is best (Taken from EKG Weekly).
STEP 1: Quickly exclude STEMI
Always prioritize rapid STEMI exclusion before exploring pericarditis-specific findings
Reciprocal ST Depression: Present in STEMI, absent in pericarditis (except ST depression in leads aVR or V1—which is expected).
STE in Lead III > Lead II: Suggests inferior STEMI; opposite typically true for pericarditis (STE greater in II than III favors pericarditis).
Horizontal or Convex Upward ST-Segment Morphology: Suggests STEMI; concave upward favors pericarditis (but does not rule out STEMI in isolation).
"Checkmark Sign” (R-T sign): Sharp upward deflection at the end of the ST segment, suggests STEMI.
New Q-Waves: Suggests myocardial infarction.
Step 2: Identify Features Suggestive of Pericarditis
PR-Segment Depression: Pronounced PR-segment depression in multiple leads, particularly in cases of viral pericarditis. This finding can be transient.
Spodick Sign: Downsloping of the T-P segment can be suggestive of pericarditis but should be interpreted with caution.
Pericardial Friction Rub: The presence of a pericardial friction rub supports the diagnosis of pericarditis.
Confirm from STEP 1: STE in Lead III > Lead II, concave upward ST-Segment morphology, STD only in aVR or V1
Let’s look at that EKG again.
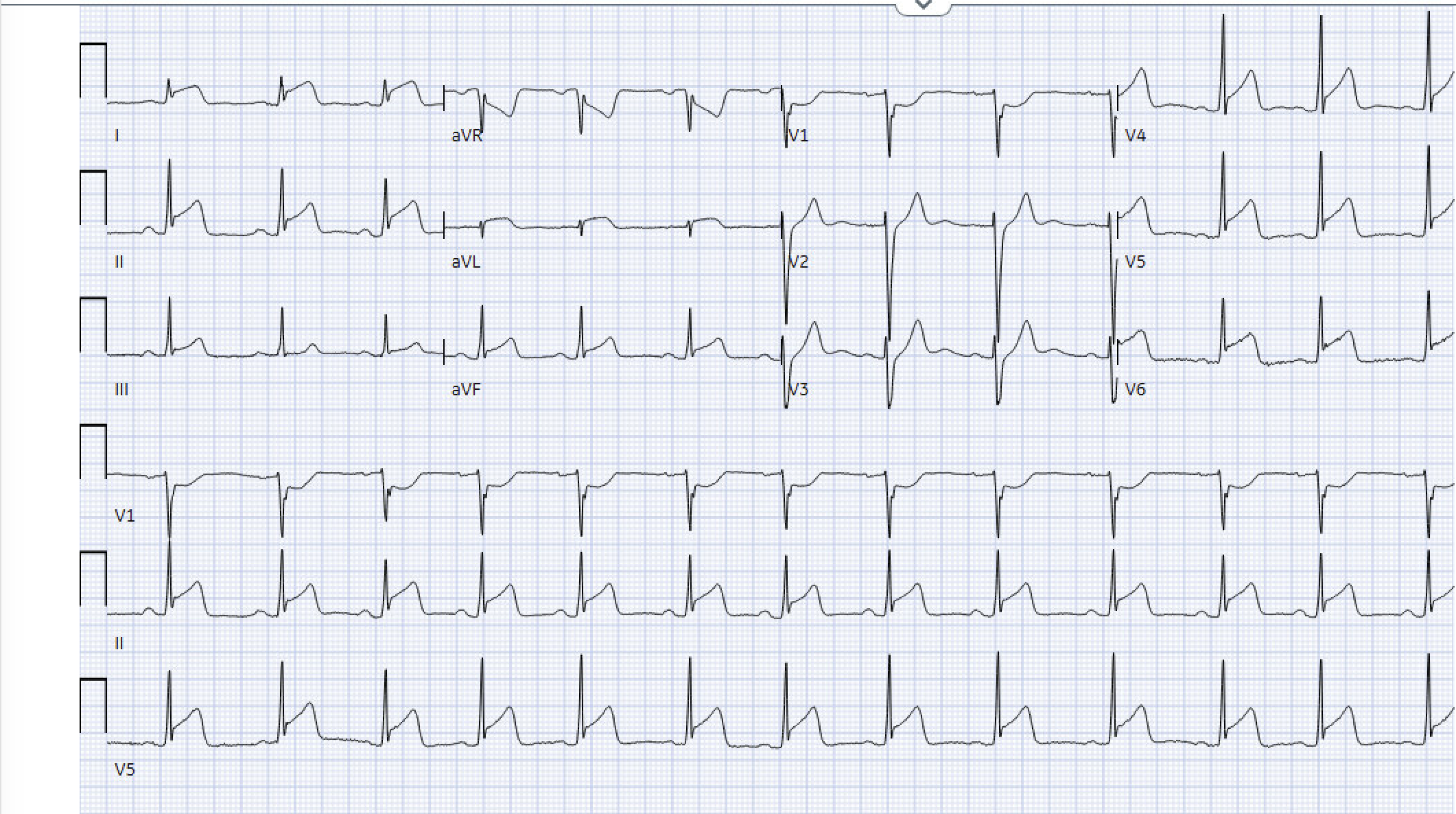
Diffuse ST elevations in a non-coronary artery distribution. Reciprocal depressions only in aVR and V1. Primarily concave upwards STE (I and AVL are a little worrisome…). STE Lead II > Lead III.
Diagnosis here leans “myopericarditis”. Especially when considering the patient’s history and exam. But… definitely get a cardiologist involved for final decision-making.
Diagnosis of Pericarditis
To diagnose acute pericarditis, at least 2 of the following 4 criteria should be met:
Pleuritic Chest Pain:
Description: Sharp, pleuritic, and/or positional chest pain that may radiate to the trapezius ridge.
Diffuse ST Segment Elevation or PR Segment Depression:
ECG Findings: ST segment elevation and PR depression in multiple leads.
Classic ECG patterns occur in less than 60% of cases.
PR depression is not a specific finding and is not pathognomonic of pericarditis
Note: These also occur in the setting of MI. This is why it’s important to first rule out STEMI on the EKG before considering pericarditis.
Classically, ECG changes in patients with acute pericarditis progress through four stages. However, patients do not necessarily present with stageable ECG abnormalities and may not progress from one stage to the next in an orderly fashion. Take these with a grain of salt.
Stage I: Diffuse ST-segment elevation that occurs in multiple leads (except for V1 and aVR) with diffuse PR-segment depression.
Stage II: The ST segment returns to baseline, and the T-wave flattens.
Stage III: The T-wave inverts, and there is potential ST-segment depression.
Stage IV: The ECG returns to normal over the course of weeks or months.
Pericardial Friction Rub:
Listen to a sample friction rub here.
Stethoscope diaphragm over the left sternal border
Often louder at inspiration, but sometimes can be better heard on forced expiration.
May be better heard when the patient bends forward or in left lateral decubitus.
The prevalence of a pericardial rub in pericarditis varies widely—It is anywhere between 35% and 85%.
New or Worsening Pericardial Effusion:
Imaging: Detected usually via echocardiography
While the finding of a pericardial effusion supports the diagnosis, the absence of a pericardial effusion or other echocardiographic abnormalities does not exclude pericarditis.
Pericarditis is a cause of tamponade—be sure to evaluate for pericarditis.
Medicolegal Risk: POCUS chest pain patients with concerning stories. Typical Chest pain + New Effusion meets the definition of pericarditis.
What is myopericarditis?
Source: ESC 2015 Guidelines for the Diagnosis and Management of Pericardial Diseases
Myopericarditis = More pericarditis, some myocarditis.
Patients meet definite criteria for acute pericarditis show elevated biomarkers of myocardial injury (ie: troponin) without imaging evidence of newly developed focal or diffuse impairment of left ventricular function. Our patient!
Perimyocarditis: More myocarditis, some pericarditis
Patients meet definite criteria for acute pericarditis, have elevated biomarkers, AND show evidence of new-onset focal or diffuse reduction of left ventricular function .
Treatment of pericarditis and myocarditis is for a different day….
Take Home
When faced with diffuse ST elevations, always exclude STEMI first before anchoring on pericarditis. True reciprocal ST depression, STE in lead III greater than lead II, convex or horizontal ST segments, Q waves, or focal wall motion abnormalities favor STEMI. Pericarditis is suggested by diffuse, concave ST elevations, ST depression limited to aVR or V1, and STE greater in lead II than III. However, no single ECG feature is definitive, making distinction from STEMI challenging. Best of luck out there!
Cheers,
Dillon