
Quick Hits: PTA and Migraine Treatment
Hey Team,
Two quick items from yesterday's shift.
1. Peritonsillar Abscess
When was your last one? Would you feel comfortable managing the next one without defaulting to CT?
There’s a solid 2022 review in Annals of Emergency Medicine worth skimming.
Why we care
PTAs are typically polymicrobial. Untreated, they can progress to serious complications including descending mediastinitis, retropharyngeal abscess, necrotizing fasciitis, and Lemierre syndrome.
Diagnosis
-Clinical diagnosis is often sufficient.
- POCUS performs well and can be done intraorally with reported sensitivities around 90 to 100 percent, or via transcervical/transmandibular approaches with sensitivities around 80 to 90 percent.
- CT approaches 100 percent sensitivity and identifies complications, but adds radiation, cost, and time.
Medical Management
- NSAIDs such as ketorolac for pain control and to help with trismus
- Single-dose dexamethasone reduces pain and may shorten recovery.
- Antibiotics: Augmentin for oral therapy, Unasyn if IV. Treat infection and prevent complications.
Medical management alone may be reasonable in select patients. There is no strict size cutoff, but patients with abscesses under 1 to 2 cm, minimal or no trismus, and who appear non-toxic may be candidates for antibiotics alone.
Drainage
The Annals review provides a clear written walkthrough.
There is also a helpful EMRAP video demonstrating needle aspiration technique.
2. Migraine Treatment
No deep dive here, but the 2025 American Headache Society guideline update on ED migraine management is worth reviewing. It may shift my own practice.
Highlights:
- Prochlorperazine now favored over metoclopramide as first-line dopamine antagonist.
- We should become more comfortable with nerve blocks, particularly the greater occipital nerve block. Check out this video demonstrating the procedure.
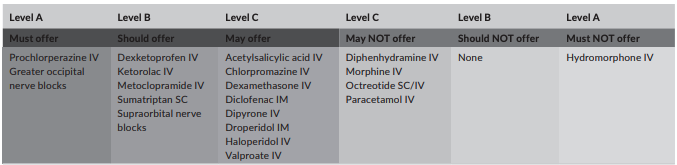
Summary of evidence table by level for all treatments from the 2025 review. Robblee 2025, Headache
Additional commentary from the guideline:
- Normal saline has no strong supporting evidence for routine use unless the patient is clinically dehydrated.
- Diphenhydramine likely does not improve pain outcomes. Consider using it for treatment-induced akathisia rather than prophylactically.
- Acetaminophen appears to offer limited benefit in this setting.
- CGRP monoclonal antibodies are emerging, but no ED-specific recommendations yet pending further studies.
Worth a quick read.
Best,
Dillon