
Post Cardiac Arrest Management
Hey Team,
I wanted to link you to several resources worth reviewing after our resuscitation a few days ago.
Tamis-Holland, J. E., et al. Cardiac Catheterization Laboratory Management of the Comatose Adult Patient With an Out-of-Hospital Cardiac Arrest: A Scientific Statement From the American Heart Association. Circulation, 149(5), e274–e295. [pubmed]
This is a scientific statement published in 2024 that has an extensive discussion regarding when and to when not to go to the cath lab.
Post-Arrest Cardiac Cath EMRAP Episode: https://www.emrap.org/episode/worstcasescenar/cardiologycorne5
This is a cardiology corner episode that reviews this scientific statement in some but not all detail.
Hirsch, K. G., et al. Part 11: Post-Cardiac Arrest Care: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 152(16_suppl_2), S673–S718. [pubmed]
This is the Post-Cardiac Arrest Chapter of the AHA 2025 ACLS/Cardiac Arrest Guidelines. Lot's of good stuff here.
Post-Cardiac Arrest Care EMRAP Episode: https://www.emrap.org/episode/paceyourself/critbitspostcar
This is a "Crit Bits" episode that reviews this AHA chapter in some but not all detail.
There is quite a bit to read through and listen to here. But definitely worth it to up your post-cardiac arrest game.
Key Points:
Post-ROSC cath lab decisions (no STE)
No routine immediate cath for all comatose post-ROSC patients without ST-elevation. Contemporary trials (e.g. COACT, TOMAHAWK) and AHA guidance support a selective strategy.
However, emergent/urgent cath is reasonable when there is ongoing concern for an ischemic culprit despite no STE: recurrent VT/VF, cardiogenic shock, dynamic ischemic ECG changes, refractory instability, or high pretest probability of acute coronary occlusion (chest pain before arrest).
Do not use early neurologic exam or perceived poor prognosis to exclude cath. Early neurologic findings are unreliable, frequently confounded by hypoxia, sedation, paralysis, and post-arrest encephalopathy, and should not drive cath decisions.
AHA “poor prognostic indicators” that could play a role in cath decision if no STE: unwitnessed arrest, non-shockable initial rhythm, prolonged no-flow or low-flow time, severe metabolic acidosis or lactatemia, advanced age, and significant comorbid illness. Importantly, the AHA emphasizes these are associations, not definitive predictors.
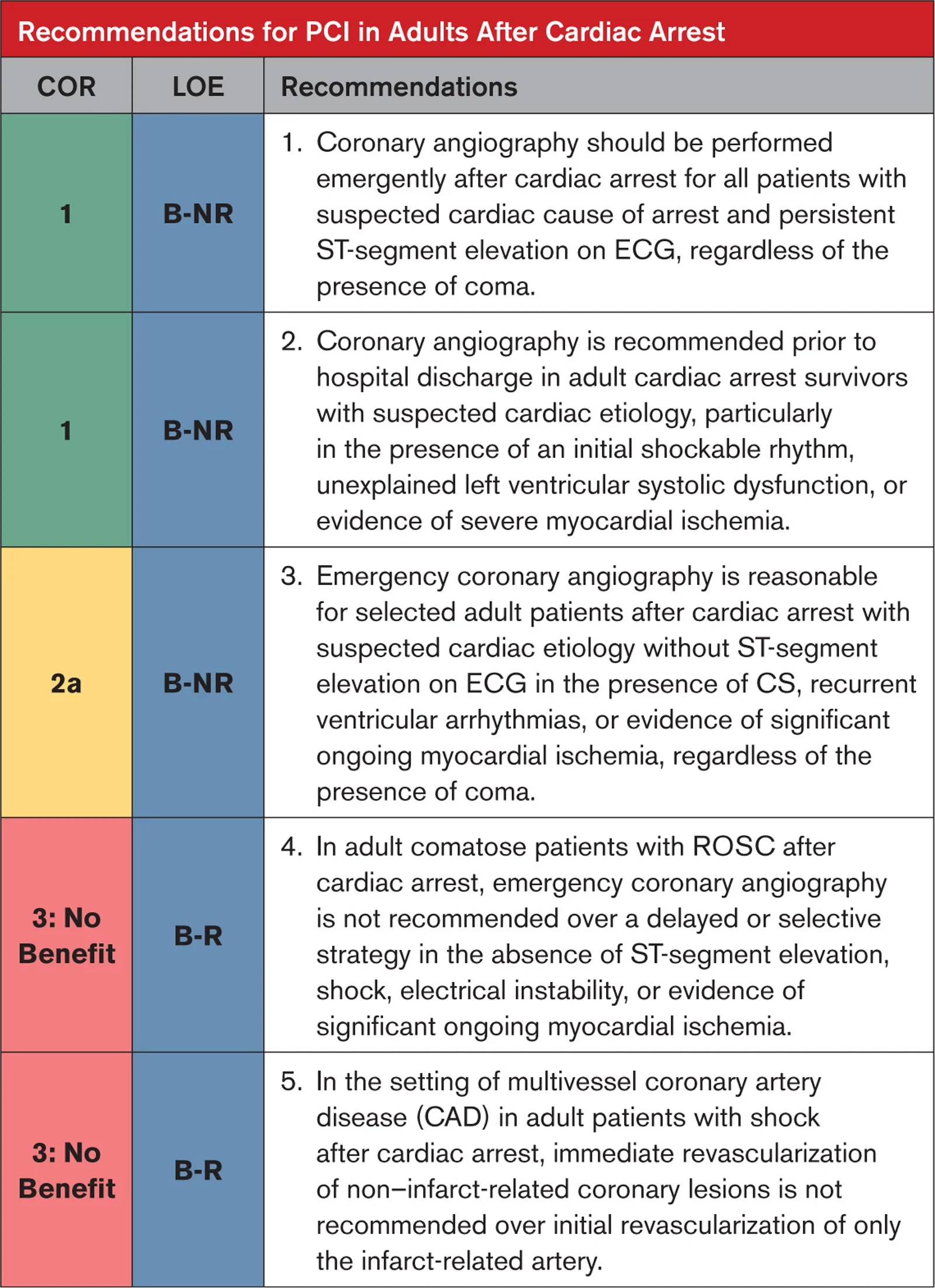
Source:AHA Guidelines 2025
Neuroprognostication pearls:
Avoid early prognostication. Formal neurologic prognostication should occur ≥72 hours after ROSC and after rewarming (If TTM used), with sedatives and paralytics cleared.
Multimodal only. Prognosis should integrate serial neurologic exams, EEG, imaging, and biomarkers. No single test or early finding is sufficient.
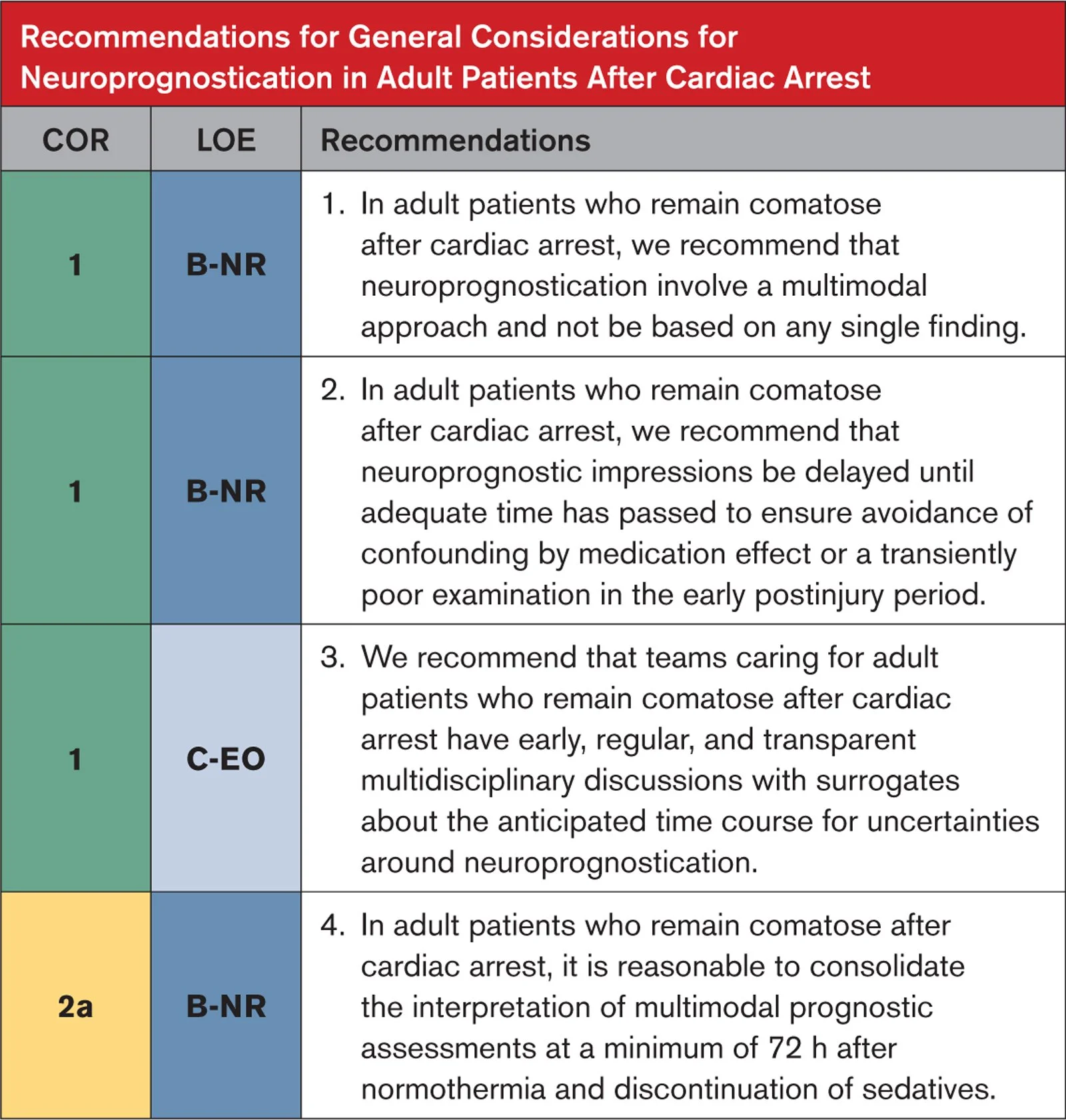
Source: AHA Guidelines 2025
Other Post-arrest care recommendations:
Physiology first. Target adequate cerebral perfusion with MAP goals typically ≥65 mmHg, avoid hypoxia and hyperoxia, prevent fever, target normocapnia, control glucose, and identify and treat seizures.
Cheers,
Dillon