
Welcome to The Pearl Log — where post-shift wisdom surfaces, one shiny clinical take at a time. Some pearls are fresh, some are rough, all are found under pressure.
Find a Pearl

Acute Diverticulitis Updates
CT with IV contrast remains the imaging workhorse, but well-appearing patients with a classic history may not always need a scan. Uncomplicated cases could skip antibiotics altogether if they’re stable, tolerating PO, and low-risk for progression. Complicated cases still require a surgical consultation.
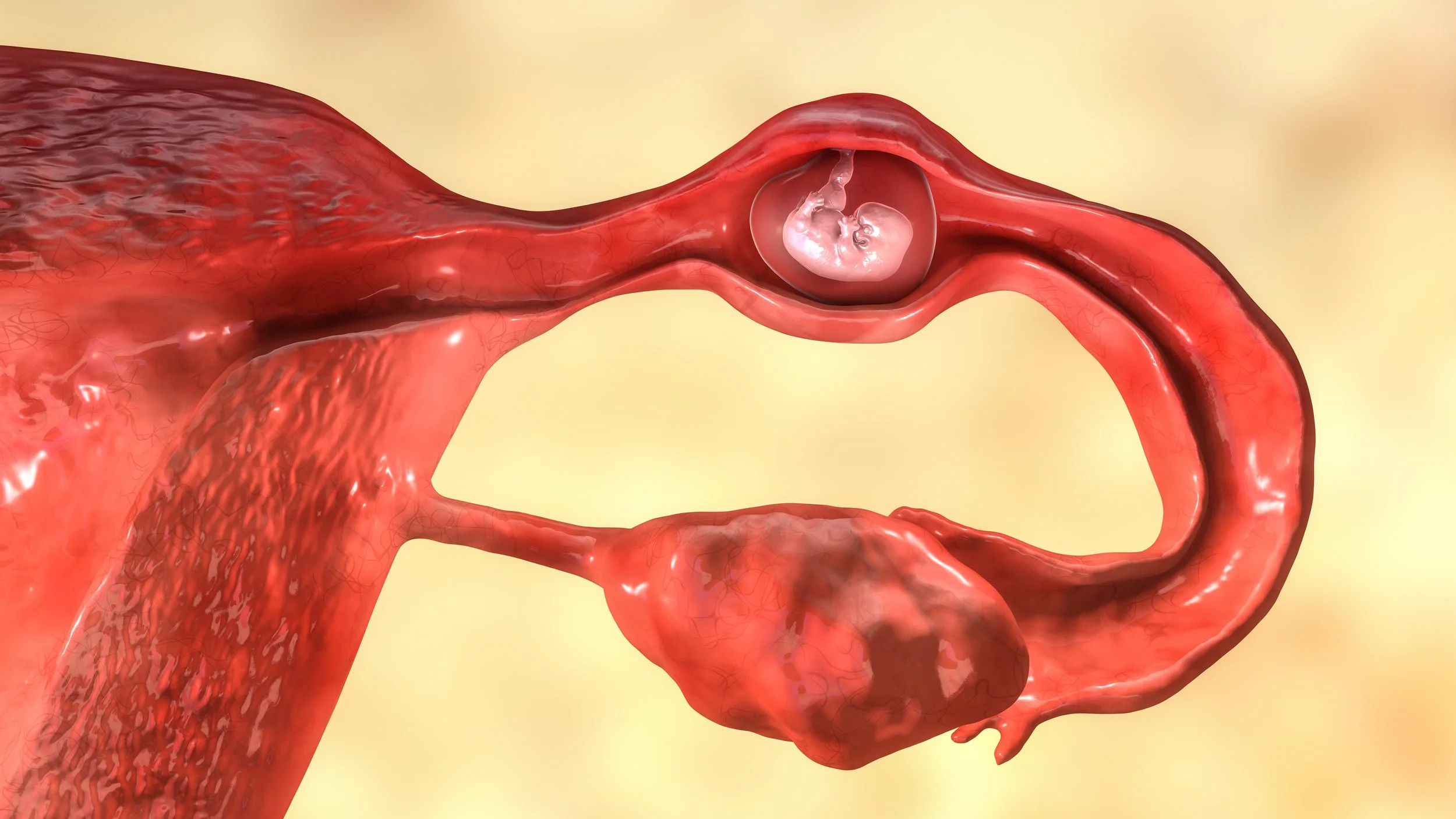
The Beta-HCG and Ectopic Pregnancy. Myth-Busting.
You can’t rule out an ectopic pregnancy with a low or “reassuring” β-hCG. The discriminatory zone only applies to normal intrauterine pregnancies, not ectopics—and many ruptures occur with levels well below 1,500 mIU/mL. Every symptomatic pregnant patient needs an ultrasound, regardless of hCG value. No hCG cutoff, and no pattern of symptoms, safely excludes an ectopic.

Diabetic KetoALKALOSIS
Sometimes DKA doesn’t read the textbook.
A patient can have elevated beta-hydroxybutyrate and a wide anion gap, yet show a normal or even alkalemic pH—thanks to vomiting, volume contraction, or mixed acid-base shifts. That’s diabetic ketoalkalosis. Don’t be fooled by the “normal” blood gas; if the gap and ketones are high, treat it like DKA.

Lactate, Lactate, Lactate…
Lactate has two personalities, and not all of them mean “shock.”
Type A stems from true hypoperfusion and anaerobic metabolism, while Type B comes from impaired lactate clearance or altered cellular processing—think thiamine deficiency, ethanol, metformin, malignancy, or liver disease. And when it spikes after a seizure? It’s only meaningful if caught fast—within about 90 minutes—before it clears and the trail goes cold.