
Leg Pain Pontification
Hey Team,
Let's talk leg pain.
1) Osteoarthritis (OA) — worth a quick reset
Take a look at this “Seminar” from The Lancet
Pathophysiology
OA reflects a multifactorial process involving genetic predisposition, biomechanical stress, obesity, and low-grade inflammation. This leads to cartilage loss, synovial hypertrophy, subchondral bone remodeling, and osteophyte formation. The gut microbiome is an emerging contributor via systemic inflammation, though human data remain limited.
Presentation
Classically presents with activity-related joint pain. Pain is multidimensional, driven not only by structural damage but also by nociplastic and neuropathic-like mechanisms from central sensitization. Psychosocial factors such as mood, coping, and socioeconomic status meaningfully influence symptom severity.
Imaging
OA is a clinical diagnosis. Imaging is not required to initiate treatment and should be reserved for atypical features or concern for alternative diagnoses.
Imaging–Pain Discordance
Radiographic severity correlates poorly with pain. Cartilage is not innervated; pain arises from synovitis, bone changes, nerve ingrowth, and central sensitization. Pause before you reflexively order an x-ray for atraumatic knee pain if the presentation seems consistent with OA.
Management
No disease-modifying therapies exist. Management is stepwise:
Education and activity modification
Exercise and weight management
Topical NSAIDs as first-line pharmacotherapy, seem to be as effective as oral NSAIDS
Joint replacement for refractory disease
2) DVT Workup — a practical framework
Think of DVT ultrasound as the “CT PE” for leg pain/swelling. Use D-dimer to guide who actually needs imaging. Not all leg pain needs an US.
Stepwise approach
Wells score to determine pretest probability
D-dimer
Standard cutoff: <500 ng/mL
Age-adjusted: age × 10 ng/mL (for patients >50)
Obtain a compression ultrasound only when indicated
Key decision points
Wells ≤2 + negative D-dimer → safely exclude DVT
Avoids imaging in ~29% of cases
<1% subsequent VTE rate
Wells >2 → go straight to ultrasound (skip D-dimer)
If negative proximal US: repeat in 1 week or obtain whole-leg US
Age-Adjust that Dimer for DVT
New data supports age-adjusted cutoff in DVT risk stratification (JAMA, Jan 2026 – Le Gal et al.)
Among patients with D-dimer level between 500 µg/L and their age-adjusted cutoff, none developed venous thromboembolism at 3 months. Use of the age-adjusted cutoff resulted in a 7.4% absolute increase in the proportion of patients in whom the diagnosis could be excluded.
See this EMA Episode about this age-adjusted article.
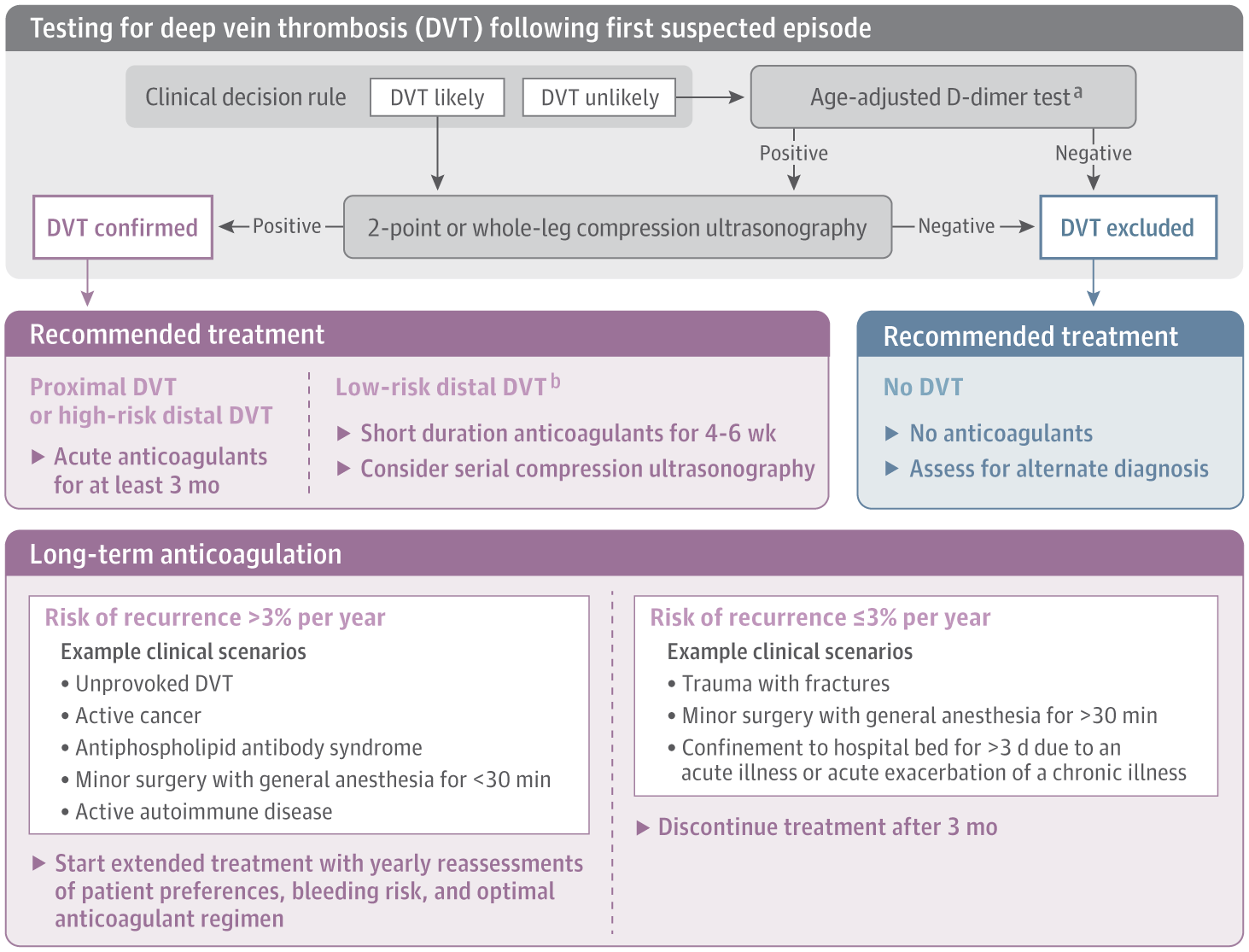
See below a Proposed DVT Diagnostic Algorithm from a JAMA Review Article in 2020.
References
Le Gal G, et al. Age-Adjusted D-Dimer Cutoff Levels to Rule Out Deep Vein Thrombosis. JAMA. 2026 Feb 3;335(5):416-424. doi: 10.1001/jama.2025.21561. [pubmed]
Chopard R, Albertsen IE, Piazza G. Diagnosis and Treatment of Lower Extremity Venous Thromboembolism: A Review. JAMA. 2020 Nov 3;324(17):1765-1776. doi: 10.1001/jama.2020.17272. [pubmed]
Ferreira Branco D, Kwoh CK, Patzer T, Loggia ML, Guermazi A, Jarraya M. Insights into the complex relationship between pain and imaging-detected structural damage in knee osteoarthritis. Skeletal Radiol. 2026 Apr 1. doi: 10.1007/s00256-026-05204-4. Epub ahead of print. PMID: 41922848.[pubmed]
Kloppenburg M, Namane M, Cicuttini F. Osteoarthritis. Lancet. 2025 Jan 4;405(10472):71-85. doi: 10.1016/S0140-6736(24)02322-5. [pubmed]