
Enough is Enough. Routine Coags in the ED.
Hey Team,
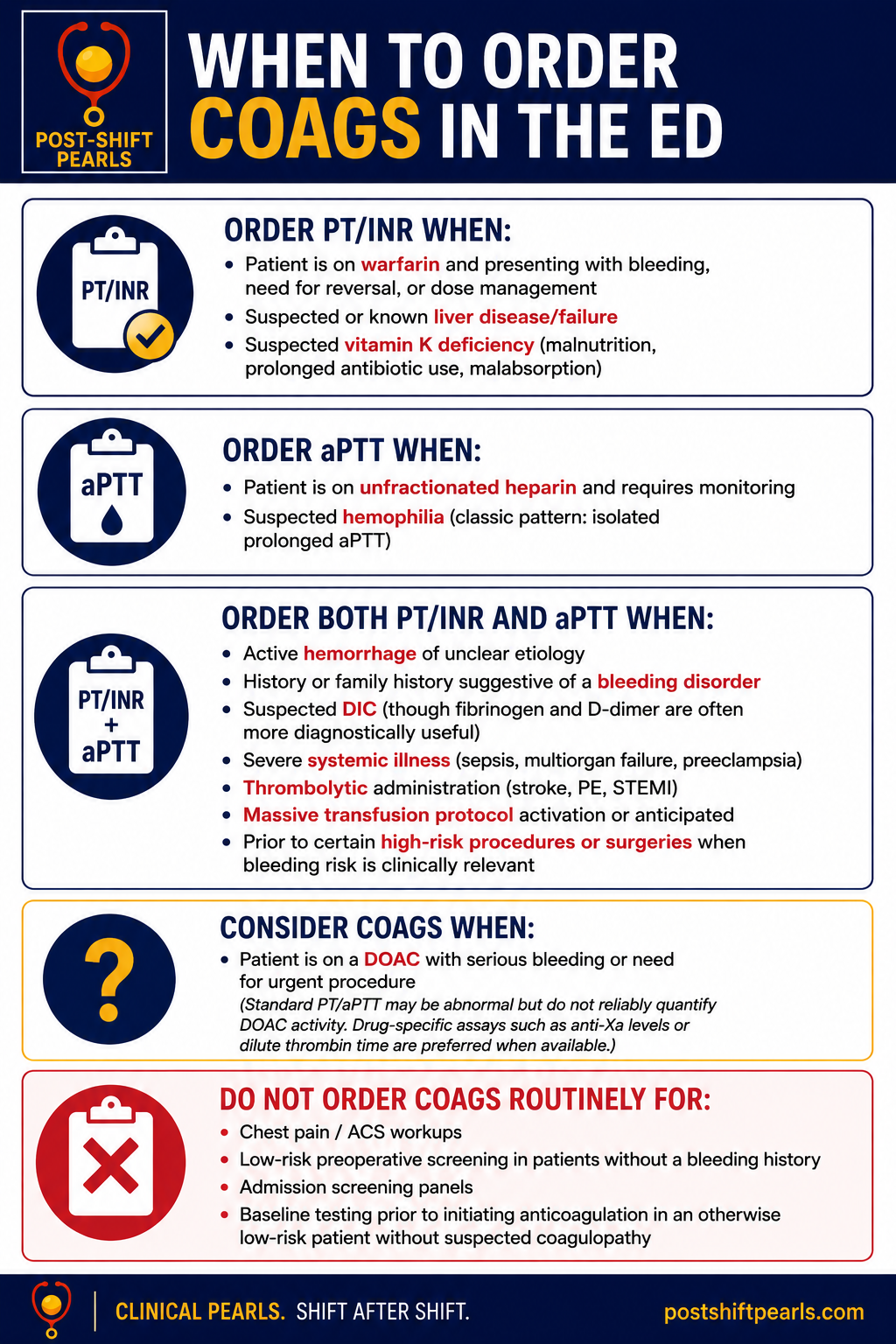
Let’s talk coags.
Bottom Line: In patients who are not bleeding, not on anticoagulants, and do not have liver disease, severe systemic illness, or a bleeding history, routine PT/INR and aPTT testing are usually low-value. A focused bleeding history is generally a better screening tool than a reflex coag panel.
Evidence Summary
Ordering routine coagulation studies on ED patients without a clinical indication is increasingly recognized as low-value care.
Multiple studies across elderly fall patients, chest pain evaluations, preoperative populations, and admitted patients have shown that abnormal results rarely change management in the absence of anticoagulant use, liver disease, active bleeding, or suspected coagulopathy.
Professional societies increasingly recommend against routine coagulation screening, instead favoring a targeted bleeding history to identify patients at risk. Recent systematic review data also demonstrate a weak and inconsistent association between PT/aPTT abnormalities and perioperative bleeding risk in most elective surgeries. The notable exception appears to be patients with advanced liver disease.
Importantly, hospitals that have actively reduced routine coag ordering through QI initiatives have done so without increases in adverse events, transfusions, or missed bleeding complications
Deeper Dives Worth a Read
For the EM-focused review, check out the AJEM article (also attached) on routine coagulation testing in the ED. The authors note that coag testing in chest pain evaluation, routine perioperative assessment, prior to initiation of anticoagulation, and as broad screening for coagulopathy in admitted patients has low utility and rarely changes management.
A recent systematic review in the Journal of Thrombosis and Haemostasis reviewed 100 studies and found a weak association between PT/aPTT abnormalities and bleeding outcomes in both minor and most major elective surgeries, reinforcing that these tests are poor general screening tools in low-risk patients.
But what’s the harm in a lil’ test?
The harm isn’t theoretical. Unnecessary coag testing in low-risk patients generates false positives at a predictable rate (~5–7%), triggering downstream workups, hematology consults, unnecessary plasma transfusions, repeat testing, and surgical delays, often without improving outcomes.
One Canadian ED QI initiative that reduced routine coag ordering estimated annual savings of $163,000 CAD across two EDs, without increases in transfusions or downstream testing.
A single-site chest pain study found nearly $17,000 spent on coag testing in 327 patients without indication, and none of those patients required a management change based on results.
Key References
Long B, Long DA, Koyfman A. Emergency medicine misconceptions: utility of routine coagulation panels in the emergency department setting. Am J Emerg Med. 2020;38(6):1226-1232.
Rahhal H, Sampat R, Tse B, et al. Assessing preoperative bleeding risk using international normalized ratio and activated partial thromboplastin time: a systematic review. J Thromb Haemost. 2026.
Capoor MN, et al. Prothrombin Time and Activated Partial Thromboplastin Time Testing: A Comparative Effectiveness Study in a Million-Patient Sample. PLoS One. 2015.
Tawadrous D, et al. Reducing unnecessary testing in the emergency department: The case for INR and aPTT. CJEM. 2020.
Kochert E, et al. Cost-effectiveness of routine coagulation testing in the evaluation of chest pain in the ED. Am J Emerg Med. 2012