
Early Pregnancy Loss in the Emergency Department
Hello Team,
We saw quite a few patients with early pregnancy loss during our last shift. I figured it would be a good time to review management.
Key References:
The 2025 Practice Bulletin by the Journal of Obstetrics and Gynecology Canada (JOGC)
The 2018 ACOG Practice Bulletin with the 2024 update on Rhogam in 1st trimester pregnancy
Early Pregnancy Loss
Big picture
Early pregnancy loss (EPL) occurs in about 15% of recognized pregnancies and is one of the most common OB presentations we see in the ED. While medically straightforward in many cases, it carries a significant psychological burden, including anxiety, depression, and even PTSD.
From an ED perspective, this is not just a diagnostic task. It is a communication task. Patients benefit from clear, direct framing: that this is common, that it is not their fault, and that most cases are due to chromosomal abnormalities and are not preventable. How this is delivered often shapes the entire experience.
Early pregnancy loss carries a significant psychological burden, and how we communicate the diagnosis matters as much as the medical management. Use clear, direct, and compassionate language, avoid minimizing terms, and explicitly acknowledge the loss while normalizing a range of emotional responses. Create space for questions, assess what the patient understands, and involve them in shared decision-making. Patients consistently identify poor communication and lack of empathy as major gaps in ED care, making thoughtful, patient-centered counseling a core part of management.
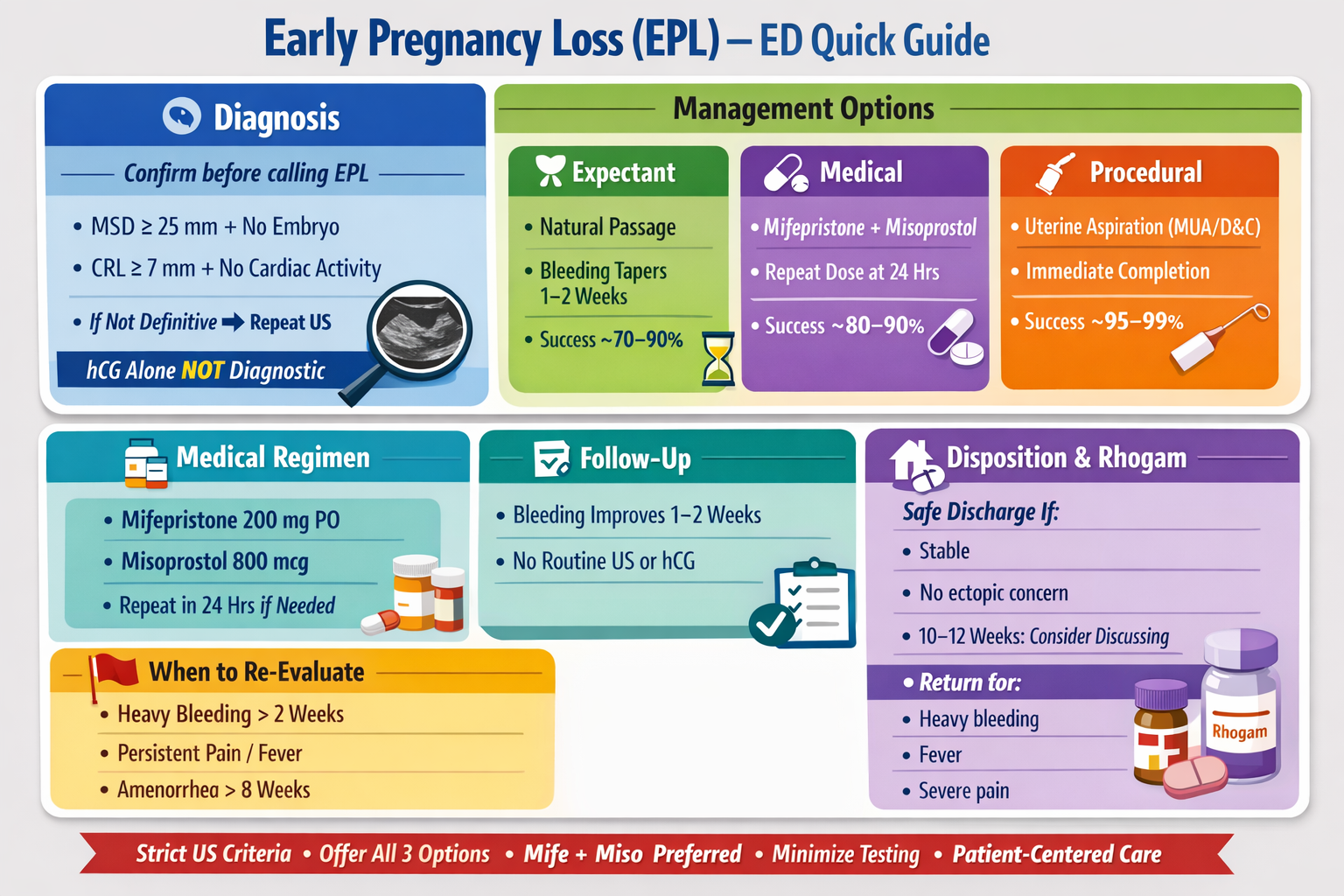
Diagnosis:
Definitive ultrasound criteria include:
Mean gestational sac diameter ≥ 25 mm with no embryo
Crown-rump length ≥ 7 mm with no cardiac activity
If these criteria are not met, the pregnancy should be considered indeterminate rather than a confirmed loss. In these cases, close follow-up and repeat imaging is the safer approach.
β-hCG values alone should not be used to diagnose EPL, given the overlap with viable intrauterine pregnancy and ectopic pregnancy.
Management overview: three equivalent options
For hemodynamically stable patients without infection, three management strategies are considered equally appropriate:
Expectant
Medical
Procedural (uterine aspiration)
One important systems issue is that patients diagnosed in acute care settings are less likely to be offered medical or procedural options. In the ED, we should at least introduce all three approaches so patients can begin informed decision-making before OB consultation or follow-up.
Expectant management
Expectant management means allowing the body to pass the pregnancy tissue naturally without intervention.
This is often a very reasonable first-line option, particularly for incomplete EPL (for example, when there is no gestational sac and only a thickened endometrium). Patients can be managed at home as long as they are stable and have reliable follow-up.
What to tell patients:
Bleeding will often become heavier than a normal period and may include clots
Cramping can be significant during passage
Bleeding typically tapers over 1–2 weeks
Success rates are approximately 70–90%, and even higher in incomplete EPL. The ED role is largely reassurance, anticipatory guidance, and safety planning rather than intervention.
Medical management
Medical management uses medications to induce uterine evacuation and provides a more predictable timeline than expectant management.
The preferred regimen is:
Mifepristone followed by misoprostol
If mifepristone is not available, misoprostol alone can be used, but it should be given as a multi-dose regimen. A repeat dose at approximately 24 hours significantly improves success compared to a single dose.
What to tell patients:
Cramping and bleeding typically begin within hours of medication
Bleeding can be heavy and is expected
This approach offers more control over timing than expectant management
Success rates are around 80–90%, with higher rates when mifepristone is included.
In Arizona, medical management of early pregnancy loss with mifepristone and misoprostol can be initiated from the ED, with feasibility largely determined by local hospital policy and follow-up pathways.
Procedural management (uterine aspiration)
Procedural management involves suction evacuation of the uterus, typically via manual vacuum aspiration or dilation and curettage.
This is the most definitive option and is often preferred when:
The patient wants rapid resolution
There is heavy bleeding
There has been failure of expectant or medical management
What to tell patients:
The procedure is brief and usually done in an outpatient setting
It provides immediate completion
Recovery is typically quick
Success rates are very high, around 95–99%.
Rhogam Update!
For pregnancies under 12 weeks, routine administration of Rh(D) immune globulin is no longer recommended based on current evidence and recent guideline updates.
Between 10 and 12 weeks, shared decision-making is reasonable, but overall the data suggest minimal risk of alloimmunization at earlier gestational ages.
It is worth remembering that Rhogam is a blood product with cost and potential downsides, so avoiding reflexive use is appropriate.
Follow-Up Care for EPL
Once EPL is confirmed and the patient is clinically stable, routine follow-up ultrasound or serial β-hCG testing is not required.
Clinical follow-up is sufficient in most cases. Patients should be counseled that:
Bleeding typically improves over 1–2 weeks
Light spotting may persist
Ultrasound frequently overcalls retained products of conception. A thickened endometrium alone is not an indication for intervention.
Further evaluation is warranted if patients develop:
Persistent heavy bleeding beyond about 2 weeks
Ongoing significant pain or cramping
Signs of infection (fever, foul discharge)
Failure to resume menses after about 8 weeks
Outside of these scenarios, continued expectant management is often appropriate.
Disposition and ED role
Most patients with EPL can be safely discharged if they are:
Hemodynamically stable
Without concern for ectopic pregnancy
Without signs of infection
Able to follow up
Clear return precautions are essential:
Heavy bleeding (e.g., soaking multiple pads per hour)
Fever
Severe or worsening pain
Syncope or lightheadedness
Bottom line
Early pregnancy loss is common, emotionally significant, and often safely managed without intervention in the ED.
Use strict ultrasound criteria before diagnosing EPL. Offer patients all three management pathways with enough context to support shared decision-making. Avoid unnecessary imaging and lab follow-up in stable patients. Recognize that expectant management is frequently appropriate. Update your practice around Rhogam use under 12 weeks. And above all, approach these encounters with thoughtful communication, as that is often what patients remember most.