
Varicoceles and Jones Fractures
Hey Team,
Two quick items from yesterday!
Varicoceles
Anatomy and why laterality matters
Varicoceles are dilated pampiniform plexus veins.
Left-sided varicoceles are far more common because the left gonadal vein drains into the left renal vein at a right angle, creating higher venous pressure.
The nutcracker effect (compression of the left renal vein between the SMA and aorta) further increases left-sided venous pressure and explains why most varicoceles are unilateral left or bilateral.
Right-sided isolated varicoceles are uncommon, since the right gonadal vein drains directly into the IVC, a low-pressure system.
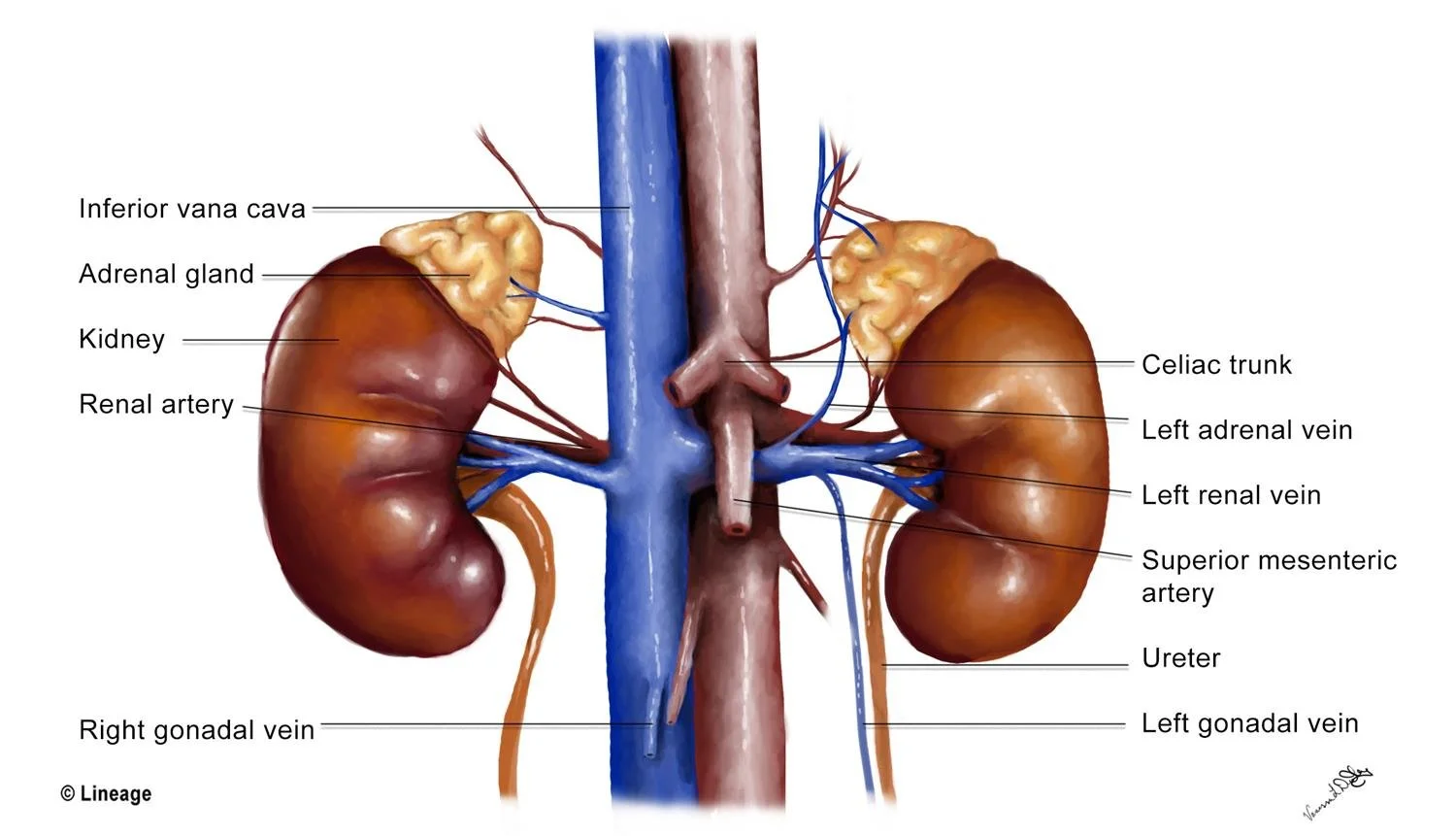
See how the left gonadal vein takes a hard turn into the left renal vein and then gets squished a bit by the SMA? The right gonadal vein has a smooth shot back into the IVC. This is what makes right-sided varicoceles rarer and more concerning. Source: Step 1 Medbullets
Clinical features
“Bag of worms” fullness above the testis, more prominent when standing or with Valsalva, and decompresses when supine.
May cause dull, aching scrotal discomfort; often asymptomatic.
Can be associated with left testicular atrophy due to increased temperature impairing spermatogenesis.
Possible association with subfertility
Diagnosis in the ED
Primarily clinical. Consider bedside ultrasound when the exam is unclear or to evaluate acute scrotal pain.
Diagnostic US findings: dilated veins ≥3 mm, increased caliber with Valsalva, and assessment of testicular volume.
When EM clinicians should worry
Isolated right-sided varicocele, especially if: new in onset, large or nonreducible, associated with systemic symptoms
These raise concern for retroperitoneal obstruction, thrombosis, or mass effect (including renal malignancy).
Initial step is scrotal US; if confirmed and suspicious, consider CT or MRI abdomen/pelvis.
Relevance to fertility
Chronic increased scrotal temperature can impair spermatogenesis.
Nonurgent outpatient urology follow-up is appropriate for fertility counseling
References:
Shridharani A, Lockwood G, Sadeghi-Nejad H. Varicocele: Clinical presentation, evaluation, and management. Rev Urol. 2017;19(2):83-89.
Leslie SW, Sajjad H, Siref LE. Varicocele. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448113/
UpToDate. Nonacute scrotal conditions in adults. Available from: https://www.uptodate.com/contents/nonacute-scrotal-conditions-in-adults?search=varicocele&source=search_result&selectedTitle=1~15
Jones vs Pseudo-Jones
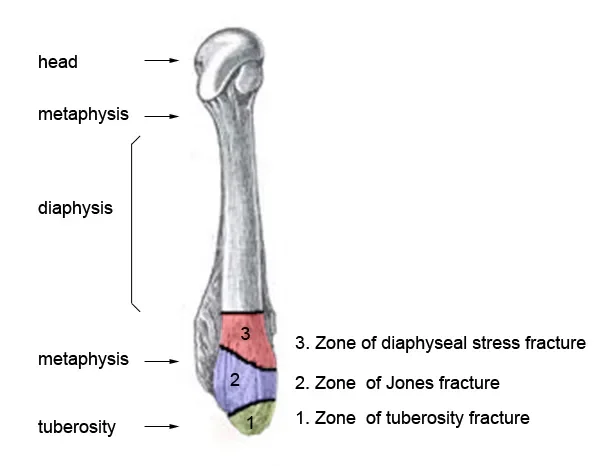
Source: Zones of the 5th Metatarsal (wikifoundry.com)
Pseudo-Jones (Zone 1 – Tuberosity Avulsion)
Avulsion off the 5th metatarsal tuberosity.
Good blood supply; low risk of nonunion.
Management
Walking boot or hard-soled shoe
Weight bearing as tolerated
Routine outpatient follow-up
Jones Fracture (Zone 2 – Metaphyseal-Diaphyseal Junction)
Fracture at the watershed vascular zone 1–2 cm distal to the tuberosity.
High risk of delayed union/nonunion due to poor blood supply.
Management
Non-weight bearing
Posterior splint or CAM boot
Ortho follow-up (early referral for athletes or high-demand patients
Misclassification often leads to premature weight bearing and failed healing.
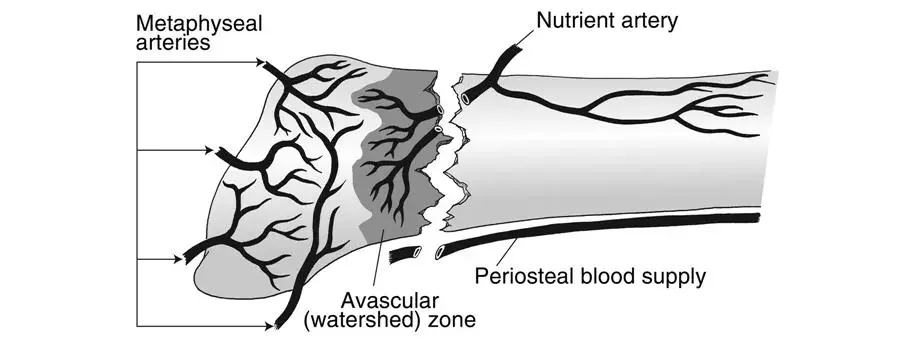
Vascular Watershed Zone (orthobullets.com)
For more information—take a look at Orthobullets – 5th Metatarsal Base Fractures and CORE EM
Cheers,
Dillon