
Tizanidine Overdose and Hyperemesis Gravidarum
Hello Team,
A couple of things from the last few shifts.
1. Tizanidine Overdose
Pharmacology
Tizanidine is a centrally acting alpha-2 agonist, similar to clonidine
Its half-life is ~2.5 hours, is metabolized by the CYP1A2 system, with a metabolite half-life ranging from 20-40 hours.
Renal impairment (<CrCl <25) and concurrent CYP1A2 inhibitors (e.g. ciprofloxacin, fluvoxamine) can precipitate toxicity at therapeutic doses
The maximum recommended daily dose is 36 mg (12 mg per dose, 3 doses/day). Any ingestion substantially exceeding this should be considered potentially toxic.
Symptoms generally appear 30 minutes to 2 hours after ingestion, with tizanidine's peak plasma concentration at ~ 1 hour
Presentation
Similar to clonidine, in that is based on alpha-2 agonism
CNS Depression: lethargy, somnolence, confusion, decreased GCS
Bradycardia, hypotension, respiratory depression, miosis
Management
Primarily supportive: close monitoring of airways, administration of intravenous fluid, and vasopressors as necessary.
DIALYSIS NOT EFFECTIVE
Role of naloxone is debated, but can consider high dose-naloxone (10 mg IV)
Clinical Course
Symptoms generally resolve within 1-3 days
Admit to a monitored bed if any are present: symptomatic bradycardia, hypotension, GCS<15, respiratory depression.
Can discharge after 4-6 hours of observation if the patient is asymptomatic
Read more about tizanidine here: https://www.ncbi.nlm.nih.gov/books/NBK519505/
2. Nausea and Vomiting of Pregnancy/Hyperemesis Gravidarum
Hyperemesis gravidarum is a diagnosis of exclusion characterized by persistent vomiting, dehydration, and ≥5% prepregnancy weight loss, with symptom onset almost always before 9 weeks
New-onset symptoms later in pregnancy should prompt evaluation for alternative diagnoses.
First-line treatment is pyridoxine (vitamin B6) with or without doxylamine, with escalation to ondansetron, metoclopramide, or other antiemetics based on severity.
Patients requiring IV hydration after prolonged vomiting should receive thiamine before dextrose to prevent Wernicke encephalopathy
Hospitalization is indicated for refractory symptoms, inability to tolerate oral intake, significant electrolyte abnormalities, or ongoing weight loss. See attached bulletin.
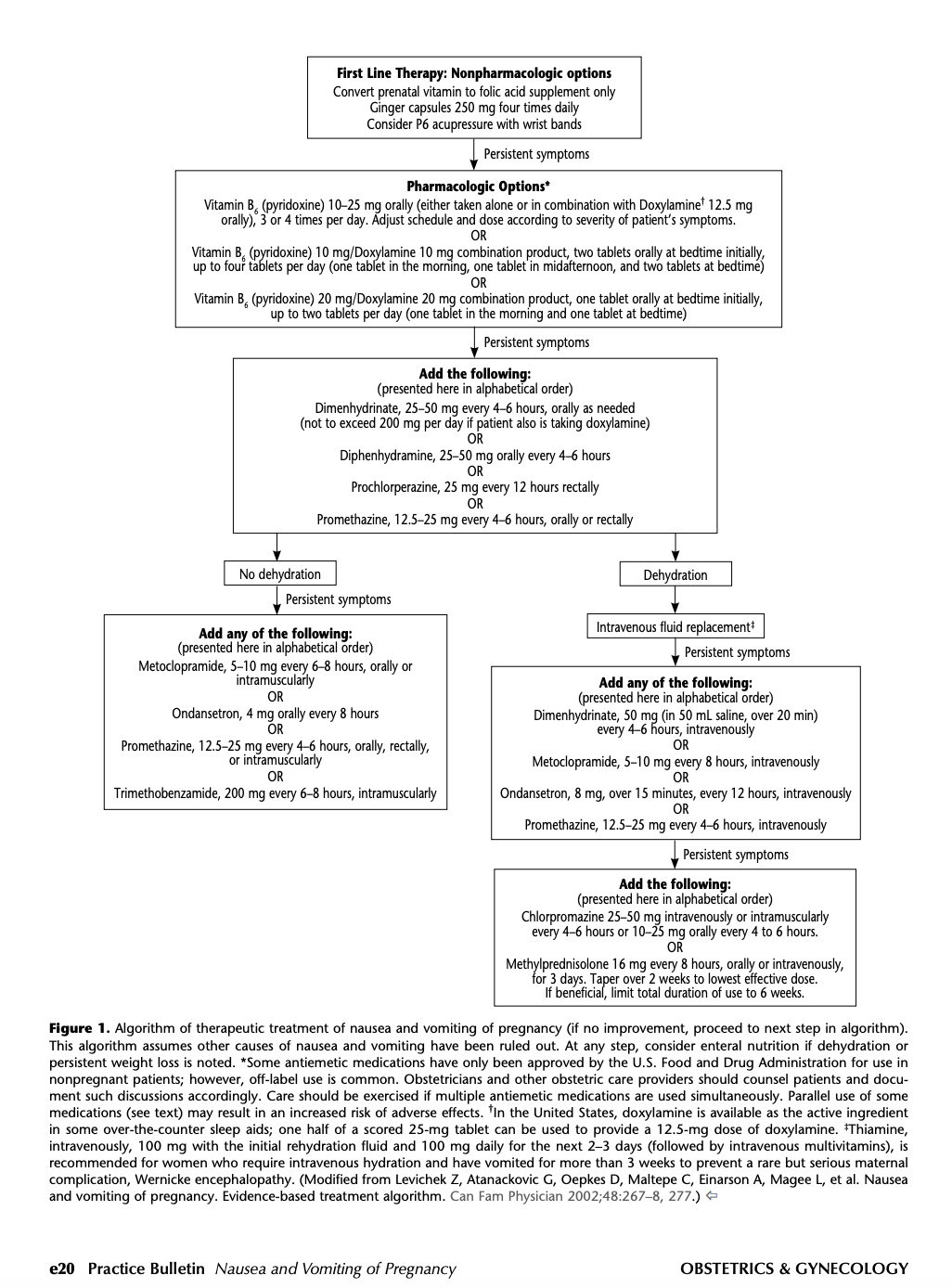
Source: ACOG Practice Bulletin 189
3. AHA PE Guideline
Don't forget to review the new AHA PE guideline
4. Check out this EM Cases Podcast Episode on Strep Throat and Antibiotics
The waters are muddy here. Based on the available evidence, antibiotics are not a benign intervention and do not guarantee clinical improvement. Tough to know what to make of it all.
If you want to deep dive, take a listen and review their show notes.
Best,
Dillon